Immediate screw-retained CAD/CAM provisionalization with an integrated digital approach
A clinical case report by Sepehr Zarrine, France
Successful immediate implant placement associated with immediate loading remains one of the biggest clinical challenges. In addition to the placement of an implant into a tooth socket concurrently with extraction, the creation of a screw-retained CAD/CAM provisional prosthetic restoration is critical for the esthetic outcome. Currently, the procedure can be achieved using a conventional approach resulting in a high number of patient appointments with time-consuming steps for the dentist. For the patient, the day of the immediate loading treatment remains a long and tiring experience from the surgery to the provisional restoration. Instead of exposing the patient to a “marathon” day, the treatment could be shortened considerably by fully involving the patient, the surgeon and the dental technician and by having a predictable treatment protocol for the tooth extraction and the prosthetic restoration design (including the individual emergence profiles prior to the surgery). This would also lead to a better patient experience and improved satisfaction. The goal of this clinical report is therefore to introduce an innovative one-step surgical approach for immediate screw-retained CAD/CAM provisionalization by using the latest technological improvements in prosthetic and surgical planning software and seamlessly integrating the dental technician into the development of the fully digital treatment planning and new prosthetics options.
Author: Sepehr Zarrine

Related topics


Initial situation
The patient was 65 years old, female, non-smoking, with a fragile health condition, and willing to get back an adequate chewing capability. The patient suffered from cachexia following a stomach ablation resulting in an obvious compromised digestion which is an aggravating factor in the dental condition (Fig. 1). The molars in sector 3 were missing, tooth 26 had to be restored and the occlusion curves adjusted. Teeth 13, 14 and 15 had a mobility classification of 3 according to Lindhe and Muehlmann. The roots were decayed and fractured, with the gum suffering from inflammation in 14 and 15 without abscess and sinusitis. Tooth 47 underwent an eruption, and bridge from 47 to 43 seems to follow this new curve of occlusion. This situation does not allow for sufficient inter-arch height in order to have number 16 as antagonist. To prevent an over-infection as well as for esthetic and comfort-related reasons, the urgency consisted in the treatment of sector 1. The overall health condition and drug treatment reinforced our decision to use a non-invasive surgical approach. The treatment plan was as follows: #47 and #43: recreating sector 4 with two individual implant-borne restorations (Straumann® Soft Tissue Level Implant RN, Roxolid® material, SLActive® surface) respecting the occlusion curves. #26: root treatment with a tooth-borne restoration in the occlusal plane. #35# 36, placing of two individual implant-borne restorations (Straumann® Soft Tissue Level Implant WN, Roxolid® material, SLActive® surface). From #13 to #16: implant-borne restoration after tooth extraction of 13, 14 and 15 (Straumann® Bone Level Implant RC, Roxolid® material, SLActive® surface) The patient will have a reduced arcade. However, the occlusion will be balanced and provide a good masticatory coefficient. The current situation forced us to compromise (Fig. 2) and to place three implants in place of three teeth: canine, premolar and molar. The aim was to extract atraumatically the three decayed teeth and to perform an immediate implant placement after extraction with flapless surgery in conjunction with immediate loading enabling restoration of the other sectors. In order to maximize accuracy and to reduce the number of steps, a fully digital approach using guided surgery was selected, allowing us to preoperatively produce a screw-retained CAD/CAM provisional restoration.


Planning
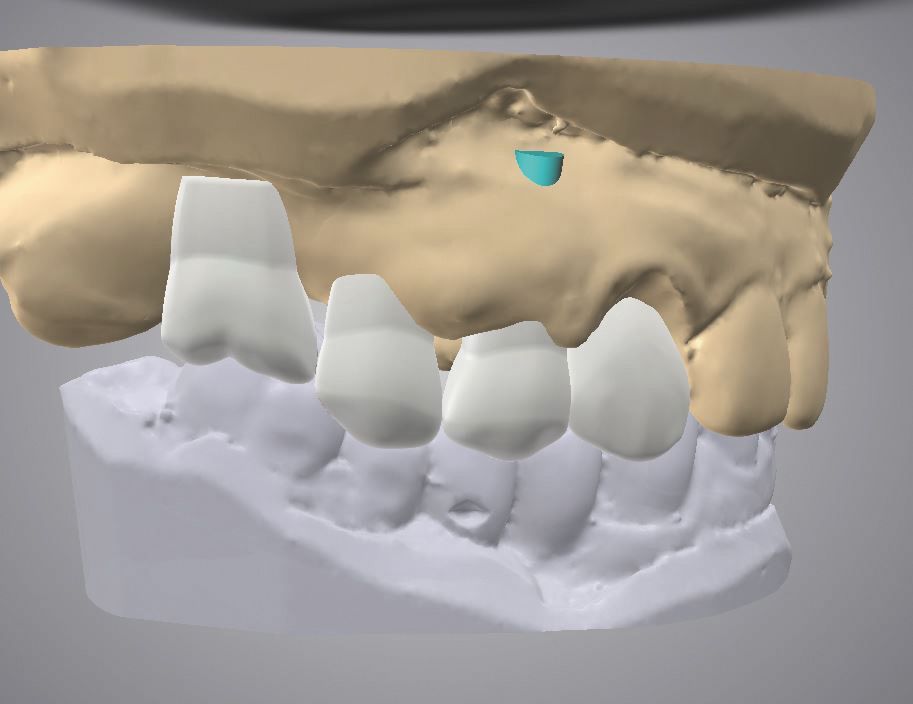
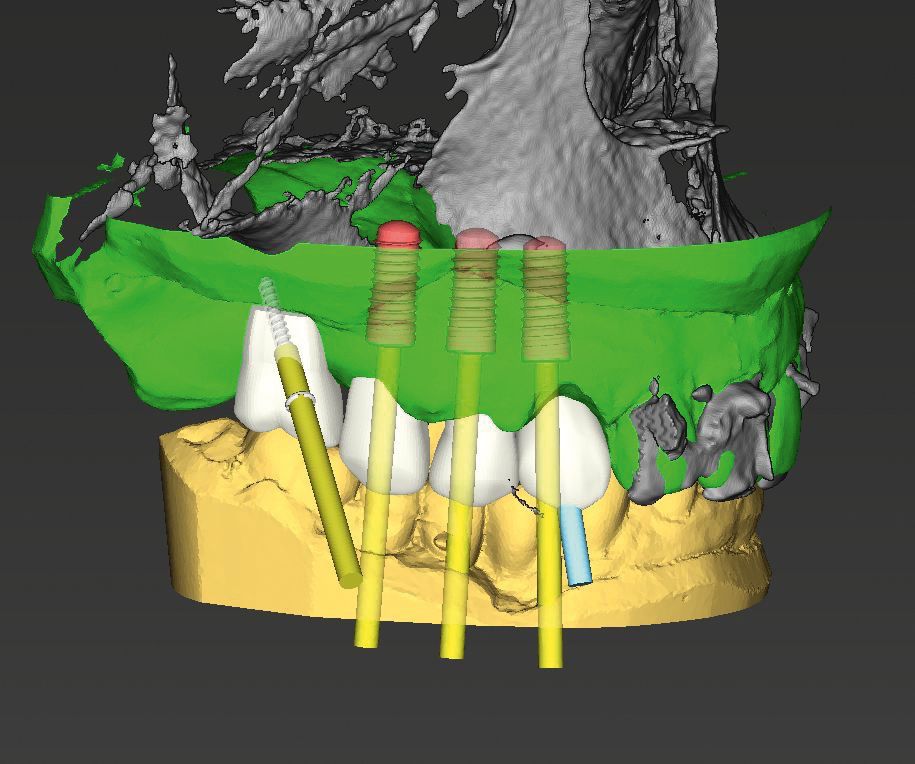
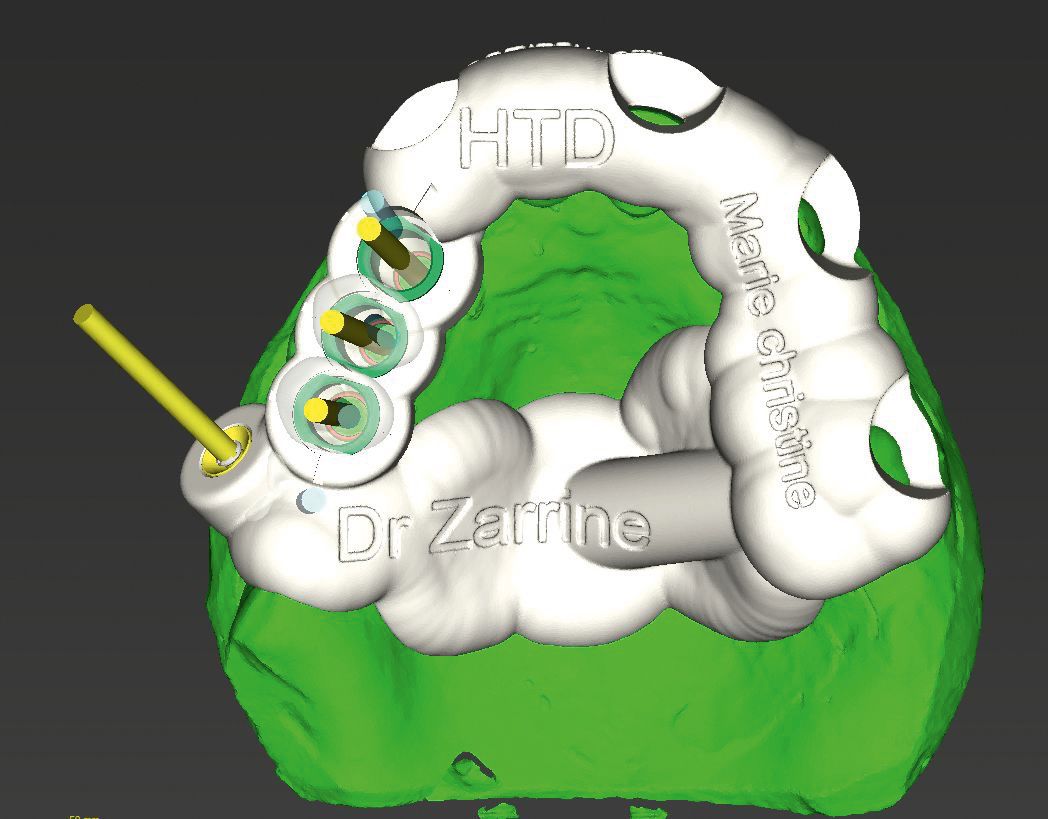
After detailed three-dimensional diagnostics, teeth 13, 14 and 15 were virtually extracted in the implant planning software (coDiagnostiX™, Dentalwings). The prosthetic design was created with Straumann® CARES® Visual (Fig. 3). The prosthetic project was shared with the implant planning software using the integrated online platform Synergy (Dentalwings). The three-dimensional radiographic DICOM data and the prosthetic design project STL file were matched in coDiagnostiX™. The integrated platform allows for real-time collaboration between the dentist and dental technician for finalizing the treatment planning from both implant placement and restorative design (Fig. 4). The surgical guide was designed with coDiagnostiX™ (Fig. 5) and produced using three-dimensional printing technology (Objet Eden260VS Dental Advantage (Stratasys, Minnesota, Fig. 6). The surgical guide was teeth- and mucosa-supported on the palate. To avoid lateral movement, fixation screws were added (Straumann® Bone Block Fixation). An individualized two-piece splinted three-unit bridge was virtually designed (Fig. 7) and CAD/CAM-fabricated from a PMMA-based restoration material cemented to a pre-fabricated bonding base (Straumann® Variobase® for bar and bridges + Polycon ae, Straumann® CARES® X-Stream™, Fig. 8 – 10). The bridge design and the occlusion were checked on a printed jaw model (Dreve Dentamid, Germany, Fig. 11) and finally sealed then sent to the dental practice with the jaw model and the surgical guides.






Surgery
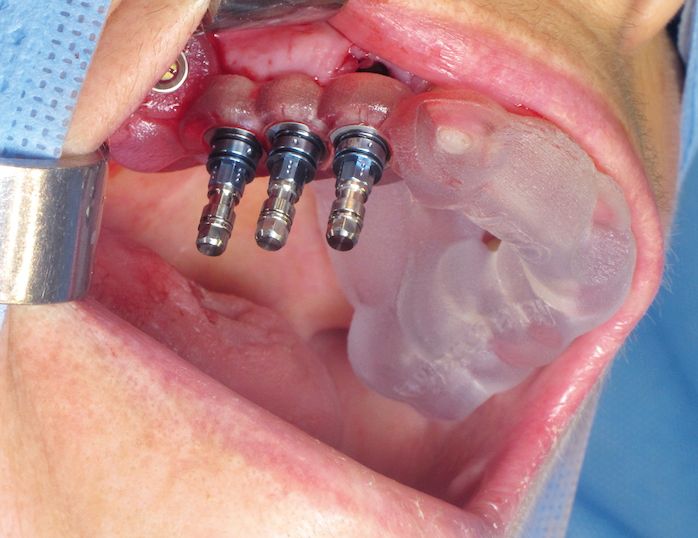
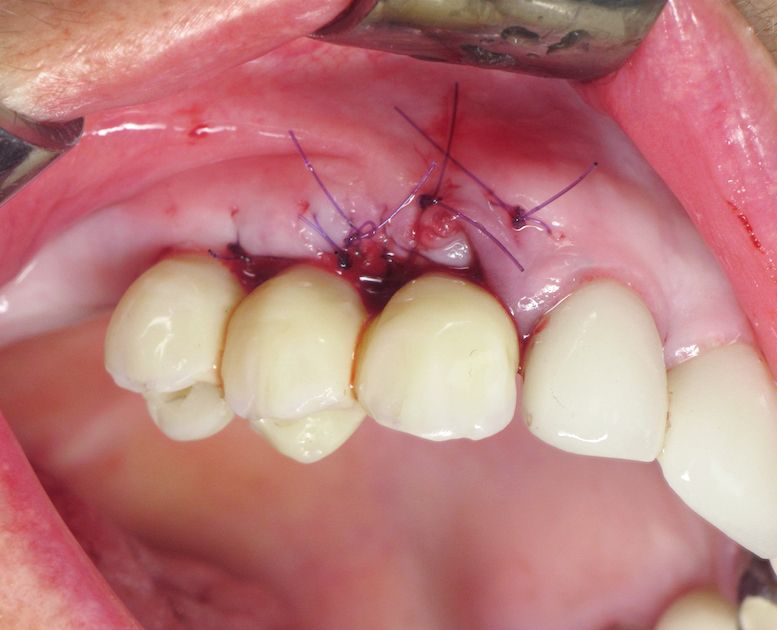
On the day of surgery (Fig. 12, 13), the surgical protocol provided by the implant planning software guides the clinician through the surgical procedure and supports him in the use of the appropriate instruments from the guided surgery surgical kit (drill heights, drill handles, etc., Fig. 14, 15). To avoid deformation of soft tissues that could influence the stability of the surgical guide, we performed regional anesthesia: Vestibular: high tuberosity anesthesia for the alveolar nerve supra-posterior, and high canine anesthesia that reaches the supra-anterior alveolar branch of the maxillary nerve. Palatal: analgesia of the nasopalatal nerve in the retro-incisive area and the large palatal nerve in the area of the large palatal foramen. The crowns were removed; the root of 13 was cut and removed in fragments. The avulsions were created delicately; the alveoli were curetted and debrided under irrigation. Papillae were detached to allow for the regularization of the bone crest by removing bone that was too thin, anticipating the post-extraction resorption. The surgical guide was placed and the position was secured using 14mm fixation screws in the maxilla at sector 17 (Fig. 16). The drilling sequences were performed through the guide. To avoid bone overheating, high irrigation was performed using the up and down drilling technique. Tapping and profile drilling were essential despite the maxillary soft bone. This is critical in order to follow all the steps necessary for correct implant positioning according to the planning. In order to maximize the precision in the implant placement, we chose shorter implants than usual. This allowed us to achieve a quicker implant positioning through the surgical guide by using guiding transfer pieces that ensured the final positioning (depth and angle). The implants were stabilized with a torque of 50 N / cm (Fig. 17). After removal of the surgical guide, the bone chips harvested during the drilling sequences were used to shape the crest and to fill the gaps. Interdental papillae were repositioned buccally by rotation. A conjunctive tissue graft was partially dissected from the palate while remaining pedicle in order to recreate the interdental papillae. Sutures helped to stabilize the gingivoplasty (Fig. 18). The screw-retained two-piece CAD/CAM bridge was finalized before surgery and immediately placed and screwed onto the three implants (Fig. 19 – 20). Slight tension was detected during the screwing, but with no consequences for the implants since they were not yet osseointegrated and the mechanical stress was too low. The only change to the temporary bridge consisted in slightly adapting the under-occlusion. Additionally, the SLActive® surface stimulates the adsorption of blood proteins and enhances the fibrin network formation, which allows for the faster maturation of the bone. This is a major asset in immediate implant placement after tooth extraction and in immediate esthetics. Check-ups at 10 days post-op (Fig. 21) and at four weeks (Fig. 22) were used to verify correct gingival healing and implant integration. The postoperative courses were not painful and no edema or hematoma was observed.









Results
Immediate implant placement associated with immediate loading is a predictable protocol with some variables. The digital tooth extraction was integrated with the production of a screw-retained CAD/CAM provisional restoration prior to the surgery and was successfully achieved and placed without any cementing steps in the dental practice. The entire treatment workflow was done fully digitally. Only a single surgical step was required to provide an entire individualized prosthetic rehabilitation.