
What is this about?
- How the Straumann® Anatomic Healing Abutment XC (AHA) can be used to shape and preserve peri-implant soft tissue in a posterior molar site.
- The role of AHA in supporting a predictable healing process and minimizing soft tissue manipulation.
- Learn about the clinical workflow and advantages of using AHA to optimize conditions for the final prosthetic restoration.
Introduction
Immediate implant placement requires careful management of both hard and soft tissues to achieve long-term stability and functional success. Preservation of the peri-implant soft-tissue contour is essential for maintaining esthetics, facilitating hygiene, and ensuring an optimal emergence profile for the final restoration. Traditional approaches often involve multiple components and appointments to shape the soft tissue and accurately capture its shape, which may increase clinical complexity and patient discomfort.
The Straumann Anatomic Healing Abutment XC (AHA) provides a simplified and biologically driven solution to these challenges. Its pre-contoured design closely replicates the natural emergence profile of the replaced tooth, thereby promoting optimal soft-tissue contouring from the moment of implant placement. This allows for minimally invasive management of the peri-implant mucosa, reducing the need for provisional restorations and supporting long-term tissue stability.
In addition to its anatomical design, the AHA also functions as a scanbody, streamlining the digital workflow. Because it can be scanned directly intraorally, there is no need to remove the abutment or introduce separate scanning components. This dual functionality helps preserve the soft tissue seal while reducing chair time and simplifying the restorative process.
The following case report presents a 65-year-old female patient treated with immediate implant placement in the mandibular molar region. It demonstrates how the use of the Straumann® Anatomic Healing Abutment XC supported soft tissue preservation, enabled efficient digital impression taking, and led to a predictable and esthetic clinical outcome.
Initial situation
The patient was a 65-year-old woman in generally good health, with well-controlled hypertension and mild obesity, and no other systemic conditions. She was a non-smoker. She presented with a crown loss on her lower right molar, leaving only the root, which made chewing on that side difficult. Her main goals were to restore proper masticatory function and maintain long-term oral health, with moderate concern for esthetics.
Intraoral examination revealed a root remnant of tooth #36, previously endodontically treated, showing secondary caries and a Grade III furcation involvement (Fig. 1).

Fig. 1
Radiographic and CBCT evaluation confirmed a vertical root fracture and failure of the previous endodontic treatment at tooth #36. Sufficient vertical and horizontal bone dimensions were observed, with D2 bone quality, indicating favorable conditions for immediate implant placement. The remaining teeth exhibited stable periodontal support and no significant bone loss (Fig. 2).
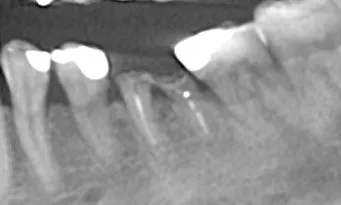
Fig. 2
The prognosis for tooth #36 was hopeless due to the root fracture.
Based on the clinical and radiographic findings, this case was classified as “advanced” according to ITI SAC criteria.
The primary objective was to restore the patient’s masticatory function through implant therapy. The AHA was used to preserve and contour the peri-implant soft tissues, ensuring their stability during healing. This approach minimized soft tissue manipulation, allowed a more predictable digital workflow, and provided optimal conditions for the final prosthetic restoration.
Treatment planning
- Immediate, non-submerged, flapless implant placement approach.
- Conservative extraction of hopeless tooth #36.
- Immediate placement of Straumann BLC™ Ø 6.5 x 6 mm, SLActive®, Roxolid® implant in position #36.
- Gap-filling using Allograft Maxgraft®.
- Digital impression with the Straumann® Anatomic Healing Abutment XC (AHA) for final restoration.
- Screw retained zirconia (ZrO) restoration cemented on a Straumann® Variobase®
- Delivery of screw-retained definitive prosthesis.
Testimonial
“The Straumann Anatomic Healing Abutment significantly reduced chair time by eliminating the need for additional steps during the soft tissue healing phase. Its pre-contoured design closely mimics the final restoration. Overall, it was a highly convenient solution that improved clinical efficiency and enhanced my patient’s experience.”
Dr. Algirdas Puišys
Surgical procedure
The patient was prepared following standard clinical protocols, and local anesthesia was administered using Ubistesin®. Tooth #36 was atraumatically extracted. After extraction, the site was prepared for implant placement by performing an osteotomy according to the manufacturer’s recommendations. A Straumann BLC™ Ø 6.5 × 6 mm SLActive® Roxolid® implant was immediately placed in the extraction socket using a flapless, non-submerged approach. The implant was placed free-hand, with careful attention to buccolingual and mesiodistal alignment. The orientation dots on the implant driver were positioned in the buccolingual direction to ensure proper positioning. Primary stability was achieved with an insertion torque of 35 Ncm (Fig. 3).

Fig. 3
An AHA XL shape with Ø6.5 WB, gingiva height 2.5 mm was selected based on the molar site anatomy and the desired emergence profile. The AHA was initially inserted with the pre-assembled self-retaining screw using the SCS Screwdriver and hand-tightened (Figs. 4-5).
Once proper fit and alignment were confirmed, the AHA was temporarily removed and replaced with a standard healing abutment to facilitate filling of the peri-implant gap. The gap was filled with Allograft Maxgraft® to support bone contour and stability. The AHA was then reinserted, with the flat scanbody feature aligned in the buccal orientation, and hand-tightened to 14 Ncm. The screw access was closed with absorbent cotton and composite restorative material.
Radiographic control confirmed proper implant and AHA positioning (Fig. 6).

Fig. 6
The surgical site was closed with sutures, and standard post-operative medications and instructions were provided. Follow-up evaluations demonstrated stable soft-tissue conditions and uneventful wound healing, confirming the predictability of the AHA-guided approach.
A Center of Dental Education (CoDE) is part of a group of independent dental centers all over the world that offer excellence in oral healthcare by providing the most advanced treatment procedures based on the best available literature and the latest technology. CoDEs are where science meets practice in a real-world clinical environment.
Prosthetic procedure
Two months post-surgery, the patient returned for the final prosthetic restoration. Before proceeding with the final restoration, the AHA was thoroughly cleaned and inspected to ensure that no visible defects were present on the scanbody feature (Fig. 7).

Fig. 7
A key advantage of the AHA is that it can be scanned directly without removal, eliminating the need for an extra scan body or additional gingival scans, as its emergence profile is already included in the design software. Scanning was performed intraorally using the Straumann® SIRIOS™ system (Figs. 8-9).
The final restoration was digitally planned, providing full 3D visualization, including critical anatomical details. This workflow enabled the accurate design and fabrication of the definitive restoration on a Straumann® Variobase® abutment, maintaining the same Consistent Emergence Profiles™ and gingival height as the AHA, with the final prosthesis produced as a full-frame zirconia (ZrO) restoration (Figs. 10-13).
Following removal of the AHA, optimal soft-tissue healing was observed. The peri-implant tissues appeared healthy, stable, and well-contoured, demonstrating successful preservation and maturation throughout the healing period (Figs. 14-15).
The definitive restoration was then screwed with a torque of 35 Ncm. Both esthetics and occlusion were carefully evaluated, and the screw access was sealed with PTFE tape and composite (Figs. 16-17).
Treatment outcomes
The AHA proved to be a highly convenient solution, eliminating the need for additional steps during soft-tissue healing. Its pre-contoured design preserved natural gingival contours and enabled precise digital fabrication of the definitive restoration. The patient achieved stable peri-implant tissue, optimal function, and a predictable outcome, improving both clinical efficiency and the patient’s experience.
Key take-aways
- The flapless, AHA-guided approach allowed predictable preservation of peri-implant soft tissue, minimizing manipulation and supporting optimal healing.
- Digital planning and intraoral scanning enabled precise fabrication of the restoration, maintaining the emergence profile and gingival contours.
- Follow-up evaluations confirmed stable soft tissue, functional success, and high patient satisfaction, highlighting the efficiency and reliability of this AHA-based workflow.