Extraordinary team wins the South Africa ITI2019 poster competition with a challenging Straumann® Pro Arch case
A distinguished team of three South African clinicians has recently won the coveted South Africa ITI2019 poster competition detailing their work on a particularly challenging case for an edentulous patient using the Straumann® Pro Arch concept. We interviewed the winning team to get some insights to their motivation and approach.

Dr Louwrens Swart BChD, MChD (MFOS), Dr Corlene Schnetler BChD, MChD (OMP), Dr Paul Van Zyl BChD, MChD (Prost) winners of the ITI2019 poster competition.

Could you please give us the background on how your team came together?
Dr Louwrens Swart: Paul and I have been friends and colleagues since university. He was my first boss in private dental practice. We both specialized (Prosthodontics and MFOS) and have been working closely together ever since. We believe in a team approach to implantology. I am very grateful to work with such a skilled clinician.
In 2018 I was approached by WIN (Women Implantology Network) to become a mentor to Corlene, a recently qualified periodontist. I accepted the challenge and became an honorary female. (I am not really sure how that impacts my life, but time will tell.) We have been collaborating on clinical and academic matters in a mutually stimulating relationship. Corlene regularly visits my practice to assist me with interesting or challenging cases.
What does the mentoring program mean for you and how has it influenced the way you work?
Dr Corlene Schnetler: As a recently qualified specialist I feel it is very important to receive guidance from more experienced clinicians. Assisting Dr Swart allowed me to gain firsthand experience of his examination, diagnosis and treatment plan processing. The practical insights gained helps me in my own practice to improve my own processes and patient treatment.
The mentoring project is a part of the WIN. Which other activities do you participate in within the WIN?
Dr Corlene Schnetler: I have been actively involved in several of the initiatives that WIN organizes around the world. In March 2019, I gave a lecture at the WIN Summit in Malta. I am the South African WIN representative and we held a breakfast in Windhoek in August. At the breakfast I gave a short talk about my personal experience with WIN and the opportunities that it has created for me. It was interesting to have discussions with other female dentists and to share their experiences. The next step would be to extend this initiative throughout South Africa.
Would you please tell us about the case poster competition ITI2019?
Dr Paul Van Zyl: The competition was hosted by the ITI Southern Africa National Congress which was held in Cape Town from 25–27 July 2019. It was a call for posters to be presented on clinical cases or research. The posters were judged by our international speakers at the congress, Prof Dean Morton, Dr Waldemar Pollido and Mr. Vincent Fermer. In total,10 posters were accepted, they were presented electronically throughout the congress. These posters were mainly from South Africa, but three posters from Jordan were also accepted. All of the accepted entries were of an exceptionally high standard. The prize was a Straumann sponsored trip to the ITI World Symposium Singapore 2020 event, including travel and accommodation for the primary author, Corlene. The ITI sponsored the World Symposium entry.
Why did you decide to take part in this competition?
Dr Louwrens Swart: Corlene assisted me during an edentulous reconstruction utilizing the Pro Arch concept, and we had very interesting discussions around the treatment plan. I urged her to present a poster in the ITI – Cape Town 2019 competition, as this would stimulate her to scientifically research our decision making on this case, thereby broadening her knowledge on the treatment of edentulism, and in this case the Straumann® Pro Arch concept. It would also contribute positively to her academic engagement in our community. The ITI conference was a very good platform to showcase this case report.
Would you please tell us more about the case you have presented? What was particularly challenging about this case?
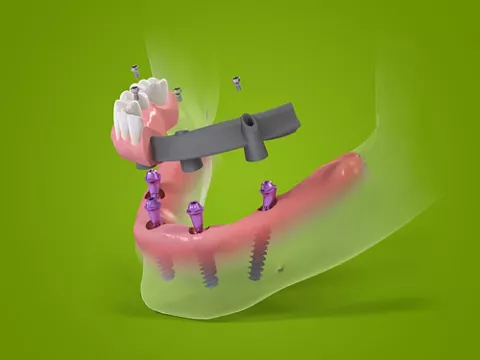
Dr Louwrens Swart: The patient requested a fixed prosthesis of the mandible to get rid of his lower denture. On examination, he had an asymmetric mandible, and different bone heights in the posterior above the inferior alveolar nerve (IAN). We opted to do the reconstruction using four implants, which is standard, but the distribution of the implants was not easy. Our primary goal was to shorten or eliminate any cantilevers, if possible.
What was your key driver to deviate from the All-on-4® concept?
Dr Louwrens Swart: The old saying “If your only tool is a hammer, every problem looks like a nail” was very true in this case. The All-on-4 concept dictates two straight implants in the anterior and two tilted implants in the posterior. If this treatment option was chosen, the needs of the patient would not have been optimally served. There was sufficient bone available for a straight implant (10 mm) in the lower right posterior mandible, above the IAN. Brunksy’s validation for tilted implants clearly states that the reason to use tilted implants is to shorten the cantilever of a fixed prosthesis. In this case a straight implant could serve this purpose much better than a tilted implant. In the left posterior mandible this approach was not an option due to the inadequate bone height above the IAN. The tilted implant option, as dictated by the All-on-4 concept, was therefore not the best available treatment choice. The Pro Arch concept solution is not restrictive in any way and allows for different treatment options in different quadrants of the jaw; thus, it was our treatment solution of choice.
Which scientific information would you use to base your decision on the position of the implant: tilted or straight?
Dr Corlene Schnetler: Dr Corlene Schnetler: According to the recent ITI consensus paper by Alccayhuaman et al there is no significant difference in implant survival rates or peri-implant bone loss between tilted and straight implants. The decision to place tilted implants is based on anterior posterior implant distribution in the arch. When there are anatomical limitations a tilted implant can increase the anteroposterior spread of the implants to reduce the distal cantilever and thus reduce the risk of mechanical complications. The maximum distal cantilever length of the prosthesis is limited to 1.5 times the anteroposterior spread and using tilted implants can help adhering to this rule. (Brunski et al) Another factor is that tilted implants can help avoid additional surgical procedures like sinus lifts or bone augmentation procedures. (Morton et al) Each patient is unique, and a patient specific treatment plan should be followed that will give the best results in the end.
For many years you have been an ITI fellow. Based on important recent scientific findings revealed in the 6th consensus paper in 2018, the recommendations have been revised, how have these recommendations impacted your treatment protocol?
Dr Paul Van Zyl: A consensus has been reached that four implants are sufficient to support a fixed prosthesis in an edentulous lower jaw. Further, consensus has been reached that an immediate loading protocol is safe to connect four implants with an interim prosthesis within a few days after implant insertion. Where the bone volume above the IAN does not allow a posterior spread of the implants, distally tilted implants are safe to use. This reduces the length of the distal cantilever on the prosthesis which subsequently reduces mechanical complications associated with distal cantilevers. In cases planned to be restored with distal cantilevers, our protocol involves immediate loading of an interim prosthesis without the distal cantilever (shortened dental arch) until the implants have successfully integrated.
In this specific case it was possible to place an implant in the posterior fourth quadrant (46 position) but we did not have sufficient bone above the IAN to place an implant in the posterior third quadrant (36). A distally tilted implant was placed only on the left in the area of the 34, to allow a shorter distal cantilever in the final prosthesis. The case was presented with the immediate prosthesis without the distal cantilever on the left.
What impact does it have for the patient and what benefits can it provide?
Dr Paul Van Zyl The patient struggled to manage with a conventional denture and did not wear it at all. We provided a new well-fitting conventional upper denture apposing a lower we replaced with a fixed interim prosthesis supported by four implants, one day after surgery. This would not have been possible without the surgery. The implant distribution was optimized to limit the risk of mechanical complications in the long term. The patient was presented with an immediate functional and esthetically acceptable solution.
What are the most important recent developments in the field of full-arch rehabilitation you see and what does the future hold?
Dr Corlene Schnetler: Digital dentistry allows increased accuracy of full-arch rehabilitations with fully guided surgical placement of implants in the correct predetermined position. It forces us to conduct better planning while providing tools to do the planning more efficiently and accurately. Improvements in the digital protocol for full-arch cases will be a focus point for the future.
Dr Paul Van Zyl Digital dentistry and the evolution of materials, has provided a vast new selection of restorative options in full-arch implant supported prostheses. In the past, cast metal substructures veneered with ceramic or acrylic came with a high incidence of technical and mechanical complications. With the use of CAD/CAM titanium substructures supporting acrylic veneering, these complications have been reduced. Together with the use of shorter and distally tilted implants, the cantilevers are reduced, which also limits complications. New prosthetic options involving the use of zirconia and the newer high-performance polymers as CAD/CAM substructures, supporting ceramic (Lithium disilicate) teeth and composite pink replacement, has opened doors which provide more esthetic full-arch, implant-supported prostheses with enhanced longevity.
Dr Louwrens Swart: Recently, the number of patients at our practice requiring full-edentulous treatments has declined significantly. The number of edentulous patients as part of the global patient population is very high; unfortunately, most of these patients do not seek dental implant reconstruction due to various factors such as limited dental education and financial means. Thus, treated cases are in decline because the population that does demand optimal treatment has a very high dental IQ—they look after their teeth well and thus require single implants for crowns or two to three implants for bridge reconstructions.
The second significant change is the number of implants used; scientific evidence now dictates that fewer implants (less than five) are sufficient for an edentulous jaw. That said, my preference is four in the lower jaw and six in the upper jaw due to the difference in bone quality of the upper and lower jaw.
The future will be dictated by digital flow guided surgery where much more emphasis is placed on the exact placement of implants to satisfy a prosthodontic-driven restoration. In this era of high esthetic demands, with dentists involved with Botox and fillers, the needs of the patient cannot be ignored. On the one hand it is commonplace to profess simple surgical options whilst on the other hand more complex treatment options are often chosen to improve the esthetic results. The forces driving these trends could be surgical capability. Many shortcomings of edentulous treatments will be visualized pre-operatively and will need to be addressed. To achieve satisfactory results, attention needs to be given to details such as nasolabial reconstruction, as well as the ease and predictability of maintenance and care for the prosthesis.