Dr. Thomas Hugh. Elevate Case of the Year Award, Winner
Background
This case outlines a female patient aged 38 Years old who presented to the surgery with considerable self-confidence issues secondary to her dental appearance. There was a history of failed interceptive orthodontics with twin block appliance therapy due to poor patient compliance, and as a result the lady possessed a retrognathic mandible and class II skeletal relationship, an underlying class II Division 1 incisor relationship with 12mm overjet and bilateral class II molar relationship
Orthodontic assessment revealed relapse was evident in the upper arch with a reduced inter-arch width in the maxillary transverse plane especially in the pre-maxilla exacerbated by the fact that the patient received maxillary second bicuspid extractions historically. There was significant rotations of the maxillary first bicuspids and first permanent molar teeth, an increased curve of Spee, mild crowding in the lower arch with early tooth wear on the mandibular incisor teeth and a lack of multiple shared posterior contacts during lateral excursions.
The patient was concerned over the amount of incisor dominance when smiling (E-pose) and wanted to widen the buccal corridors through tooth alignment. The patient had very defined aesthetic goals in mind and how she wanted to achieve them, and we felt conjointly that ClearCorrect aligners and digital smile design could provide the means of attaining a comprehensive restoratively driven outcome from the treatment. The patient declined referral to a specialist orthodontist considering her previous experience and failed earlier interventions.
This case would be considered complex due to camouflaging a skeletal discrepancy, the overjet (over 4mm) the degrees of rotation for the upper bicuspids and first molars (over 15 degrees) and the inter-arch width reduction on the maxilla. The case was managed exclusively using ClearCorrect aligners with supplementary auxiliary coupled-force continuous closed-loop elastics, to provide an improved aesthetic appearance through upper arch expansion, yet moreover a functional and stable occlusion.
I felt the benefits of ClearCorrect was the potential for clinical advisor support throughout the treatment with effectively one-to-one mentorship when troubleshooting was required during the treatment planning process and when prescribing refinements – a standout feature when considering opting for ClearCorrect over other aligner systems competitors on the market.
The patient wanted an efficient and aesthetic means of tooth movement, with the flexibility that conventional fixed appliances do not offer. Considering the history of poor compliance, we wanted a more patient-friendly modality of treatment which ensured oral hygiene was not compromised offering a significant advantage in maintaining periodontal health and reducing the risk of caries such as enamel demineralisation (white-spot lesions) around fixed orthodontic brackets. The patient also desired the shortened treatment time and for the aligners to be as discreet as possible. We planned for the ClearCorrect UNLIMITED option considering the treatment complexity, giving us the reassurance and flexibility if we encountered compliance issues, or teeth not tracking and treatment not progressing as planned.
ClearCorrect Doctor Portal showing uploaded records and treatment simulation following careful planning in conjunction with the Clinical Advisors:
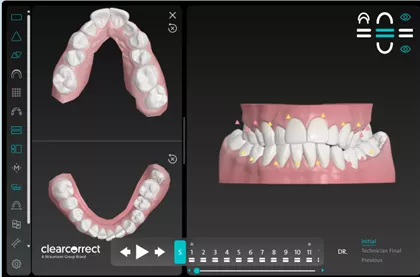
Image 1. Initial Position
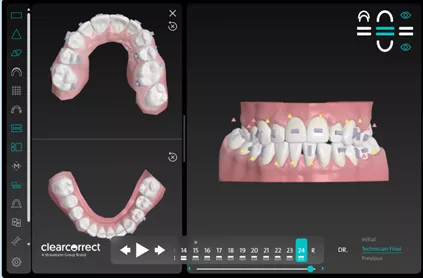
Image 2. Planned Final Position
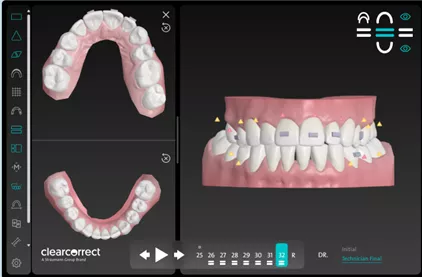
Image 3. Revision
The strategy for treatment was centred around correction of the crowding in the maxilla and mandible and reduction of the overjet through a combination of arch expansion, proclination and inter-proximal reduction (IPR). We wanted to provide symmetry to the final gingival zenith position in order to replace the interim bonding present on the maxillary central incisors with ceramic work and remove the unsightly lateral incisor additive ceramic veneers with bonding. Prior to submission of the prescription to the doctor’s portal, we placed interim composite bonding for the maxillary central incisors to work as a reference point for the incisal edge position at the end of alignment to guide final restoration length and form. Treatment was completed on a non-extraction basis. Accumulative IPR was performed between teeth: UL23 (0.3mm), UL34 (0.5mm), UL46 (0.5mm), UL12m(0.3mm), UL1-UR1 (0.3mm), UR12 (0.3mm) and UR23 (0.2mm) using a QwickStrips kit for straight contact points and Eagle Dental IPR burs for posterior sites, with the volume of reduction confirmed with a Strauss IPR gauge.
There were customised engagers (composite attachments) placed on the following teeth: UR64321, UL12346, LR34 and LL1345, this was combined with coupled force elastics with cut-outs and buttons placed on the palatal surface cervical area of the first premolars and molars in the upper arch. To mitigate periodontal ligament overload and tooth instability and unpredictability, we slowed-down the velocity of tooth movements by prescribing a maximum of 2 degrees rotation per step in the aligner sequence. All movements were cross-referenced with the ClearCorrect movement predictability chart
A wear protocol of one week per aligner was selected, yet the first aligner in the series was worn for two weeks to enable to patient to become accustomed to aligner wear, adapting to insertion and removal of the appliances and to implement strict home-care and dietary routines.
The result was achieved through a total of 32 aligners, requiring one refinement to provide more stable posterior inter-occlusal contacts and provide more bicuspid show/widening of the smile in E-pose due through maxillary arch expansion (Inter-canine width increased form 28.4mm to 32mm in total). On the whole tooth movements expressed through alignment matched the predicted outcome in the initial setup.
Cumulative rotations achieved thorough the treatment were: UR6 36o distal, UR4 37o distal, UL4 30o mesial and UL6 23o distal, overjet reduction by 4mm was achieved (12mm to 8mm) and anecdotally a pre-operatively diagnosed left sided disc displacement with reduction symptoms/signs settled completed with a complete absence of clicks/cracks and deviations on maximal translocation of the condyles.
Although not gold standard from an orthodontic perspective, I feel from a GDP’s perspective this case highlights the importance in considering past exposures to treatment and addressing the patients concerns from the outset and demonstrates how clear aligners can be used to treat relatively complex malocclusions when the cosmetic strategy has been planned form the beginning.

Figure 1. Baseline status of maxillary dentition, showing collapsed inter-arch width and V-shaped arch form, rotations of the first premolars and molars bilaterally, with severe contact point displacement in the anterior dentition

Figure 2. Occlusal view of the maxillary arch mid-treatment during first series of aligners with coupled-forced elastics in situ aiding de-rotations of the premolars and first molar teeth. Providing a more rounded arch-from and increased arch width.

Figure 3. Final arch form following alignment prior to definitive restorations for the central incisors and UL2.
Restorative workflow
Once the occlusion was finalised some failing posterior composites replaced with new conformative direct class II restorations as there was evident marginal staining and microleakage occurring. De-bonding of the engagers was performed under light detection with GC D-light pro to ensure minimal resin remained at engager sites which could stain/de-mineralise in the future.
Extrinsic tooth whitening was then completed integral to the final series of aligners using the Boutique 6% Hydrogen Peroxide daytime gels for 90 minutes over a 2-week period. The patient attained a BL4 shade with Ivoclar shade guide, forming the basis for the proposed composite and ceramic work.
To produce the central incisor veneers we optimised the restorative process by utilising a fully digital workflow, grabbing the STL files from the ClearCorrect Doctor portal of the final aligner in the series and transferring these to the laboratory along with clinical photographs for the dental aesthetics to harmonise with the facial aesthetics. The ceramic work was completed by Tautvydas Butkus at Smile Design laboratory in Elsmere Port.
The preparations for the central incisors were kept within enamel to reduce the pulpal sequelae and to provide greater predictability within bond strength between the feldspathic porcelain and resin composite. The veneers were bonded in situ under rubber dam using TransOpal IPS empress flowable nano-hybrid composite and the left maxillary incisor bonded freehand with BL-L enamel and dentine shades.

Figure 4. Bonding of digitally designed feldspathic ceramic laminate veneers to improve the aesthetic value of the maxillary ‘social six’ teeth, giving a hyper-realistic result.
The patient was provided with the option of direct composite bonding to close the black triangles between the mandibular central incisors, or further refinements with overcorrection incorporated into the aligners, yet declined both as she was happy with the cosmetics and being able to pass inter-proximal brushes through the contacts.
Upon cosmetic treatment completion, we provided the patient with ClearCorrect removable vacuum-formed retainers to prevent de-rotations and orthodontic relapse, for use indefinitely. We had discussed the possibility of fixed retainers, yet considering the experience we have opted in the short-term for close follow-up and consented the patient for future provision should this be necessary. The patient was educated on homecare and maintenance and informed to be vigilant for signs of orthodontic relapse.
Who Can Provide ClearCorrect?
To become a ClearCorrect provider, you should be a GDC registered dentist or Orthodontist. We provide various training and onboarding plans depending on your level of experience. ClearCorrect provides continuous training and support to our providers.
Interested in becoming a ClearCorrect Provider? Complete the form below to arrange a discovery call:
Frequently Asked Questions
Questions others have asked.