





















INTEGRAL guided surgery and Axiom X3® Bone Level implant for immediate protocols.

Dr Océan Fumery
Doctor of Dental Surgery
- Attached to the Department of Maxillofacial Surgery in Amiens
- Postgraduate diploma (DU) in Oral and Maxillofacial Implantology, Paris XII
- Private practice Surgery, periodontology, exclusive implantology
- Director of Study club ITI Amiens
Case introduction
In 2021, a 68-year-old healthy non-smoker presented for consultation seeking aesthetic treatment. Clinical examination revealed stage III grade A periodontitis, requiring immediate treatment. The patient’s adherence to the treatment plan led to a quick stabilization of the condition. A year later, the patient’s esthetic needs were readdressed. A digital plan was created to correct the supraclusion by reducing the overbite of the maxillary incisor block and discussed with the patient. The project was incorporated into the coDiagnostiX® implant planning software. The treatment proceeded with the immediate replacement of the avulsed teeth with dental implants, installation of multi-unit abutments, and placement of a temporary bridge. This surgical procedure permitted immediate esthetic improvements and formation of optimal emergence profiles. After four months of healing, preservation of anatomic emergence profiles was verified, and a permanent trans-screwed bridge was secured.
Initial situation:
1. Radiograph of initial situation

2. Images of initial situation, (a) anterior smiling and (b) profile view of extra-oral view showing incisor overbite.


3. Initial situation intraoral view: (a & b) absence of 11, compensated for by an amovable prosthesis. (c, d, e), simulation of the prosthesis project in the Exocad software. (f), superposition of the prosthesis project file onto an initial photo of the patient.






Treatment planning:
4 a. (a) Matching of the DICOM and the STL files with the prosthesis project in coDiagnostiX®. (b-c) plan of the implantation in respect to the residual bone volume post avulsion for optimal stability. Choice of multi-unit abutment depending on gingival height. Choice of sockets according to the implant diameter to avoid interference with the remaining teeth. (d) 5th visualization of the screwing well exits depending on the prosthesis project.
Surgical procedure:
5 a. Atraumatic avulsion. Note the presence of thick periodontal biotype with a keratinized gum band of more than 3 mm.

6. Positioning of the surgical guide and verification of its fit and stability.
7. Drilling protocol: The bone mill was used to shape the bone, preventing contact between the subsequent drill and bone. First, the pointer drill was used to mark the drilling axis and restrict propulsion into the avulsion socket. Subsequently, the Ø 2mm initial drills were used in the following order: 4.5L, 6.5L 8L and stopped at 12L. This was to ensure good primary stability for aesthetic application.
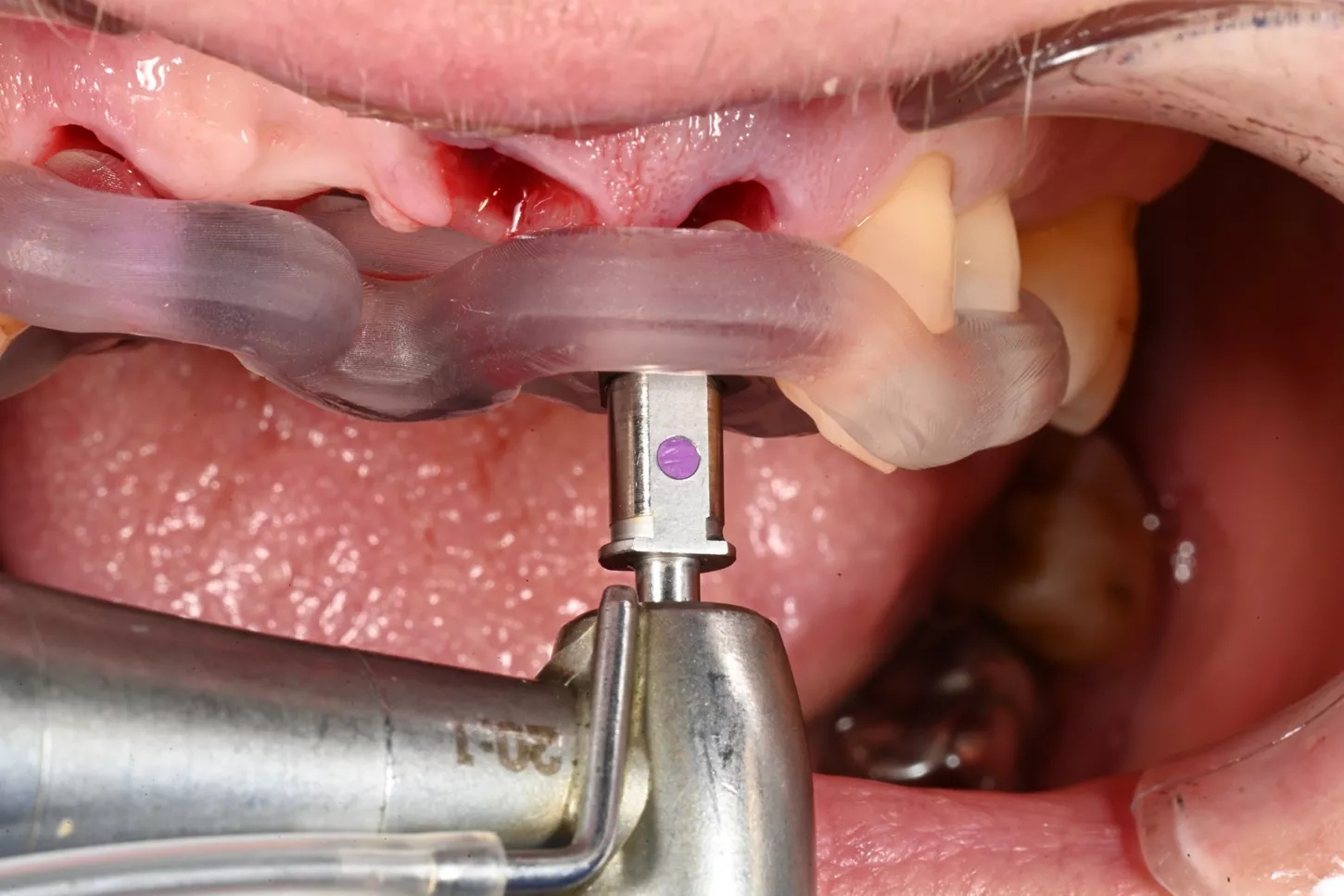
8. Implantation of the Axiom® X3 BL, size Ø3.4 mm x 12mm length in a full guided manner, until the horizontal and vertical axes are aligned on the implant holder and the guide.
9. Installation of the multi-unit pillars as planned in coDiagnostiX®. Note their insertion of at least 1.5 mm under the gum to allow adjustment of the emergence profiles.
10. Installation of the multi-unit abutment protection caps to avoid dispersion of filling particles into the threading of the abutment. Filling done using Straumann® XenoGraft, size 1000-2000 microns.
Prosthetic restoration:
11. Temporary restoration with a bridge secured using stable positioning wings on the remaining teeth. The latter is bond to the temporary abutment using self-polymerizing resin. Placement of impression transfer rods in the abutment and injection of resin around it between the temporary abutment and the bridge to easily create a screwing well.
12. Verification of emergence profiles and absence of malocclusion on the bridge 15 days post-operation.
13. Removal of the temporary bridge to record the emergence profiles.
14. Scan body placement for digital records and plan of multi-unit abutment positioning.
15. Registration of temporary bridge in place.
16. Final bridge fitting.

17. Final situation after screwing the bridges at 15 N.cm.




.png?fmt=webp-alpha&wid=1450)
Conclusion:
INTEGRAL guided surgery enables the planning of complete procedures, allowing for preservation or remodeling of emergence. Thanks to its high degree of predictability, it is now possible to prepare indexed provisional prostheses before the operation, whether for single or small-scale multiple reconstructions. The Axiom X3® BL implant, featuring a self-tapping profile and tapered apex, ensures optimal engagement in the borehole, maximizing the preservation of residual bone.