





















Digitally Driven Minimally Invasive Solution for Upper Premoler Tooth Replacement.

Dr. Giuliano FRAGOLA
Qualified Specialist in Oral Surgery
Spain
- DDS, MS, PhD Madrid Complutense University 1995
- Master science in implant dentistry 1996
- Quintessence Spanish translator and reviewer
- ITI Senior Fellow – Anthogyr national and international speaker
- External clinical Advisor Anthogyr at Straumann Group digital projects
- CEO Immersive Dental Experiences IDE. Virtual Reality dentistry apps
- Dental surgeon. Private practice Madrid, Spain
Case introduction
Immediate implant placement in single‑tooth extractions is predictable when supported by a controlled digital workflow. Preservation of soft tissue and maintenance of the emergence profile remain critical to aesthetic success [1–4]. Digital planning with coDiagnostiX® enables accurate, prosthetically driven implant positioning and fully guided surgery [1–4]. Evidence from in‑vitro and clinical studies shows that scannable healing screws or combined healing‑abutment/scan‑body systems can achieve clinically acceptable trueness/precision when appropriate scan strategies are used [5–7], and that customized/preshaped anatomic healing abutments help preserve buccal soft‑tissue contours and improve early aesthetic indices compared with conventional cylindrical healing screws [8,9]. In this context, preshaped, stock scannable anatomical healing screws—such as Healfit® SH—allow the same component to shape peri‑implant soft tissues and function as a scan reference directly in the intraoral impression, thereby reducing disconnections and streamlining data capture [5–7]. Additionally, titanium healing abutments demonstrate soft‑tissue compatibility comparable to zirconia, PEEK, and veneered zirconia without increased inflammation [10]. The X‑Base® Ti‑base then provides a seamless link from surgery to CAD/CAM restoration, enabling a plan–place–scan–restore pathway that reduces clinical steps, enhances reproducibility, and improves communication between surgical and prosthetic phases [3]. The following case illustrates immediate upper premolar replacement using this minimally invasive digital protocol.
Initial situation
A 78-year-old male in good general health, with no medication and a negative smoking history, presented with mobility of the maxillary right second premolar (tooth 15) (Fig 1a. 1b). Clinical examination revealed severe occlusal wear, plaque accumulation, subgingival calculus, bleeding on probing, and multiple carious lesions. Periodontal assessment showed probing depths >10 mm and grade III mobility. CBCT confirmed circumferential vertical bone loss around tooth 15 and generalized periodontal involvement, indicating a hopeless prognosis and the need for extraction (Fig 1c).
1a. 1b. 1c. CBCT and panoramic views showing severe bone loss around tooth 15, confirming hopeless prognosis.

1a

1b

1c
Treatment planning
Based on clinical and radiographic findings, a phased approach was adopted:
- Phase I: Initial periodontal therapy (scaling, root planing, caries management) and oral hygiene reinforcement, followed by extraction of tooth 15 once inflammation resolved.
- Phase II: Ridge preservation with xenogenic graft and membrane to maintain volume for future implant placement.
- Phase III: Digital implant planning using coDiagnostiX® for guided placement of an Axiom Bone Level implant with Healfit® SH healing abutment and simultaneous connective tissue grafting to enhance peri-implant stability (Fig 2 a&b, 3 a-c).
- Phase IV: Prosthetic workflow with digital impressions and CAD/CAM fabrication of a provisional crown, followed by definitive zirconia restoration after successful evaluation.
- Phase V: Enrollment in a supportive periodontal and peri-implant maintenance program.
2a. 2b. Implant and Healfit® SH planning in coDiagnostiX®.

2a

2b
Surgical procedure
Phase I & II: Extraction and Ridge Preservation
Tooth 15 was atraumatically extracted using a flapless approach under local anaesthesia (4% articaine with epinephrine 1:100,000). The socket was debrided and grafted with xenogeneic particulate bone substitute (Straumann® XenoOss Plus) and covered with a resorbable membrane (Straumann® MembraFlex™), secured with 5-0 non-resorbable sutures for tension-free closure. Pre- and postoperative medication included amoxicillin, ibuprofen, and chlorhexidine rinses. Healing was uneventful; sutures removed at 14 days.
3a. 3b. 3c CAD design of the tooth-supported surgical guide in coDiagnostiX®. Superimposition of the guide on the 3D bone model for fit verification prior to fabrication.

3a

3b

3c
Phase III: Guide design (Fig 3a. 3b. 3c) for guided Implant Placement and Soft-Tissue Augmentation
After healing, implant placement was performed using a tooth-supported surgical guide under local anaesthesia. A limited buccal flap allowed visual control and creation of a pouch for a connective tissue graft. Osteotomy was completed with the Integral surgery kit, and a 3.4×12 mm Axiom® X3 implant (XT34120) was placed under fully guided conditions with a Healfit® SH (OPSHSC23) healing abutment connected. A palatal connective tissue graft was positioned buccally to enhance soft-tissue thickness. The flap was sutured with 5-0 interrupted and mattress sutures. Postoperative care mirrored Phase I, with uneventful healing observed (Fig 4 a&b).
4a. 4b. Lateral view showing Healfit® SH healing screw connected to the implant and occlusal view of sutures for tension-free closure.
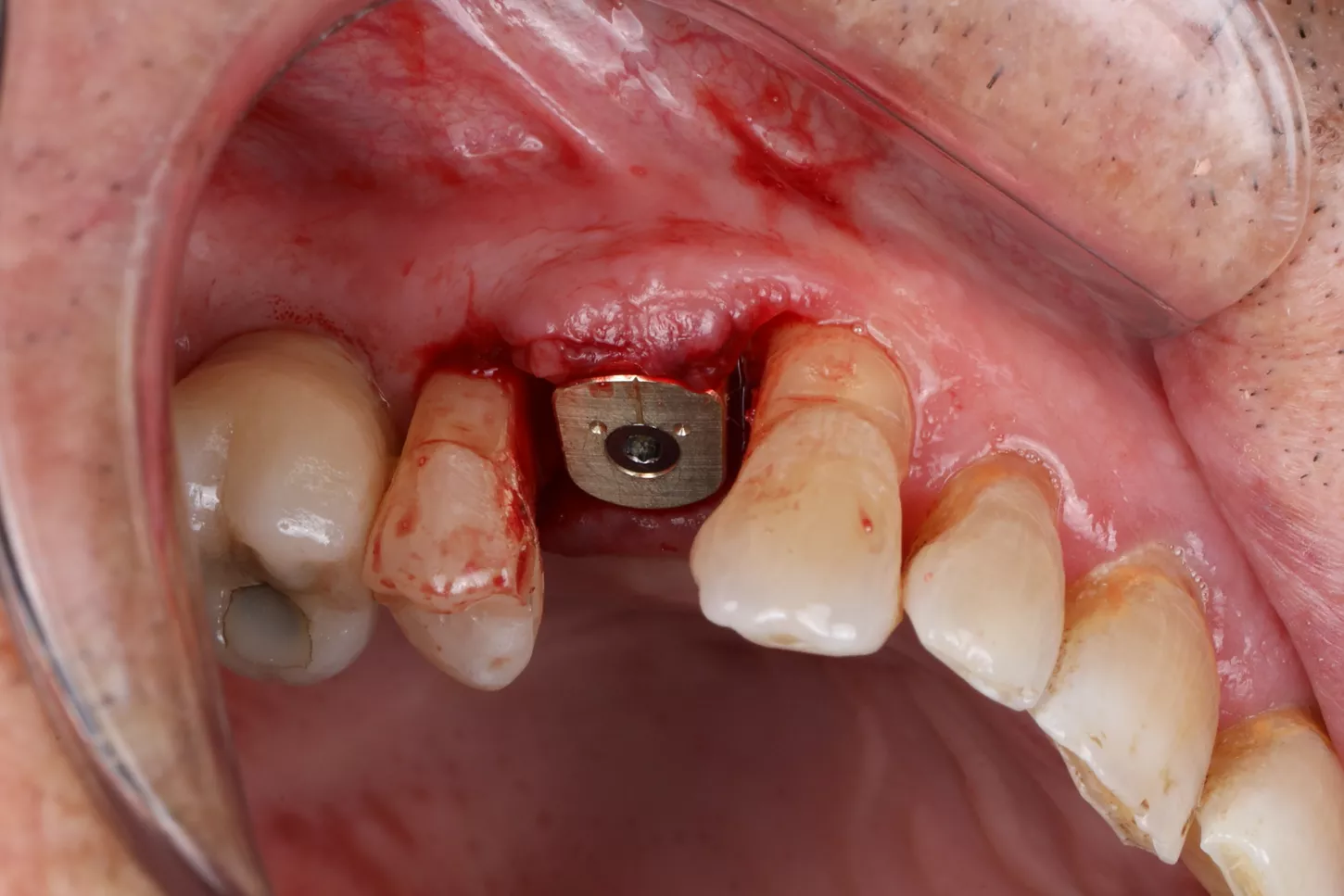
4a
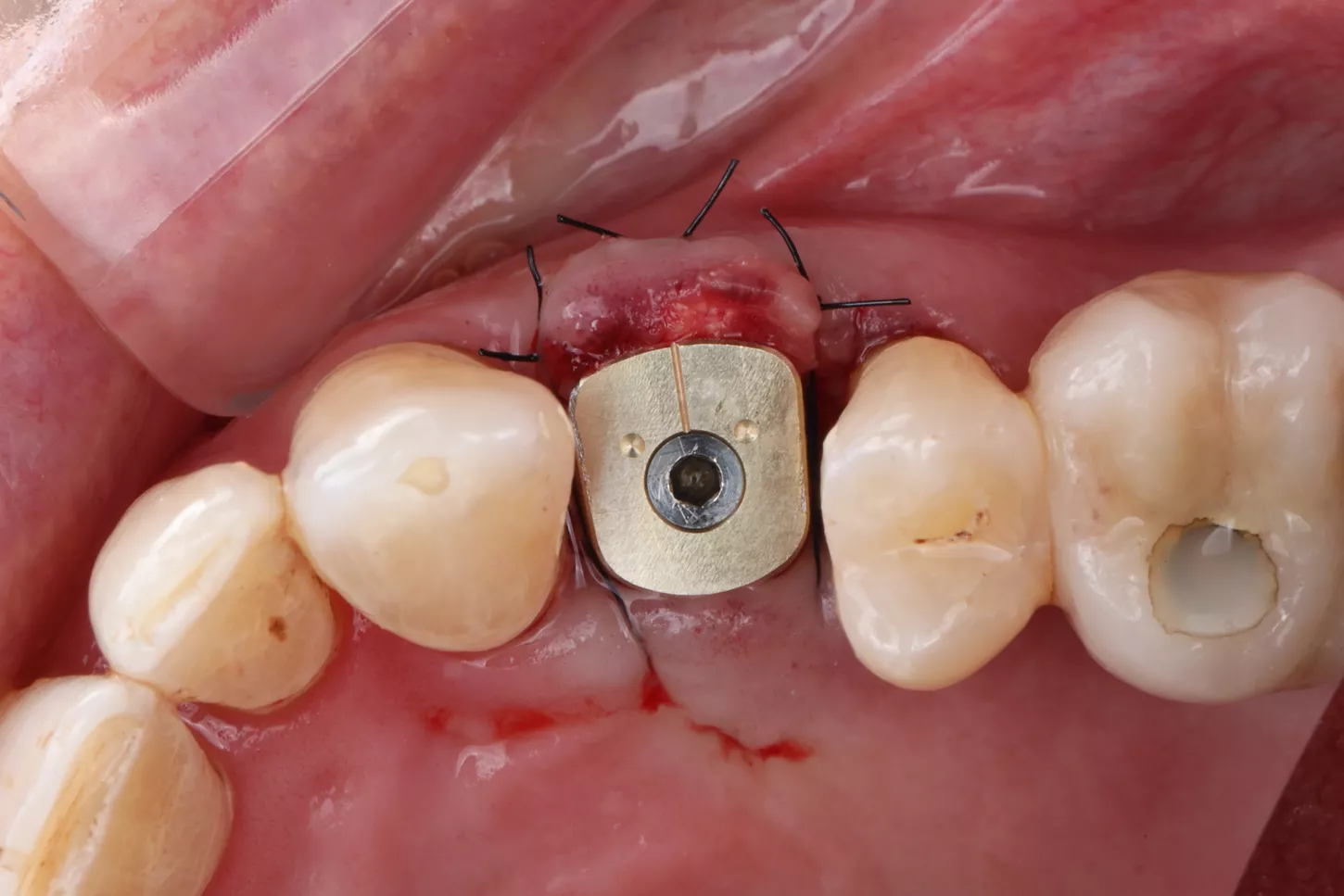
4b

Healfit® SH for optimal tissue shaping?
A 3‑in‑1 solution that preserves the biological seal and recreates a natural emergence profile thanks to its 5 anatomical shapes.
Prosthetic procedure: from digital impressions to final restoration
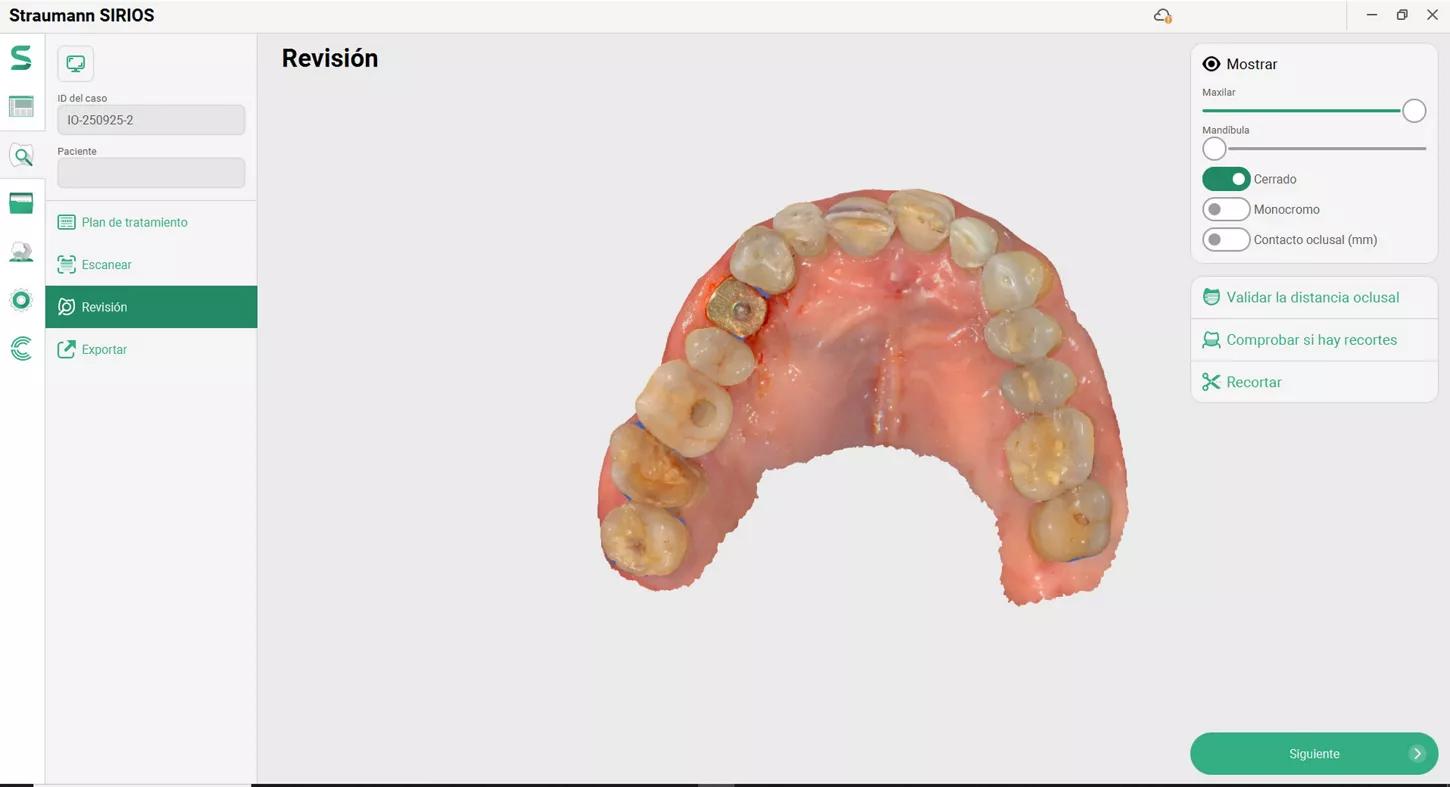
Phase IV: After a 2-month osseointegration period, delayed loading was initiated. A digital impression was captured directly on the Healfit® SH healing abutment acting as a scanbody, minimizing abutment disconnections and reconnections thus preserving peri-implant tissue integrity (Fig 5 a-d & 6).
The implant site was scanned (Straumann SIRIOS™ X3), and STL files were used to design a single crown on an X-Base® Ti-base (OPFLEX526). A long-term provisional crown was 3D-printed in resin, cemented extraorally, and delivered with adjusted occlusion for 6 months to monitor tissue stability and function (Fig 7-9) .
Following successful evaluation, a definitive monolithic zirconia crown (3Y-TZP) was CAD/CAM milled, bonded to a new X-Base® (Fig 11a. 11b. 11c), and delivered after removing the provisional restoration. The prosthetic screw was tightened to 25 N.cm, occlusion verified, and follow-up scheduled at 6 months.
5a. 5b. 5c. 5d. Intraoral scan captured with Healfit® SH acting as a scannable healing screw.

5a

5b

5c
5d
6a. 6b. Healfit SH removal using manual wrench and pre-shaped emergence.

6a

6b
7. Selection of the appropriate X-Base® Ti-Base corresponding to the healing screw using the manufacturer's compatibility table.

7
8a. 8b. 3D-printed temporary resin crown delivered with adjusted occlusion for 6-month tissue and function monitoring.

8a

8b
9a. 9b. 9c. Healfit® SH abutment and provisional crown maintaining a constant emergence profile and temporary crown placement at position 15.

9a

9b

9c
10. Panoramic radiograph showing graft healing and provisional restoration delivery at 6 months.

10
11a. 11b. 11c. X-Base® try-in before cementation, showing zirconia crown adaptation to the Ti-base and BiCopy of the provisional crown for the final restoration.

11a

11b

11c
Treatment results
Phase V: At delivery of the definitive restoration, peri-implant tissues around tooth 15 were healthy and stable, with a harmonious emergence profile, adequate buccal thickness, and no signs of inflammation, bleeding, or recession. Continuous use of the Healfit® SH abutment from surgery through impression preserved soft-tissue contours by minimizing disconnections (Fig 6a & b).
Radiographs confirmed stable crestal bone levels without peri-implant radiolucency (Fig 10). The 3Y-TZP zirconia crown exhibited light centric contacts and smooth lateral guidance, integrating well into occlusion without discomfort. Aesthetically, the crown blended naturally with adjacent teeth, and the patient reported high satisfaction (Fig 12a & b). Maintenance visits showed improved plaque control compared to baseline, supporting long-term stability and prognosis.
12a. 12b. Intraoral view of the final prosthesis in place: X-Base® abutment supporting a 3Y-TZP crown at position 15.

12a

12b
Author’s testimony
This case highlights the benefits of a fully integrated digital workflow for single-tooth implant rehabilitation in a compromised patient. Guided surgery combined with continuous use of Healfit® SH as a scannable healing abutment and the X-Base® restorative platform streamlined the transition from surgery to prosthetics and reduced appointments.
Direct digital impression on Healfit® SH preserved soft-tissue stability and emergence profile, while a CAD/CAM long-term provisional crown provided a controlled phase to assess hygiene, occlusion, and aesthetics before delivering the definitive 3Y-TZP crown.
Overall, the protocol ensured precise implant positioning, soft-tissue management, and prosthetic design, offering a predictable and efficient approach for aesthetic and biologically stable outcomes.
References
1. Hanozin B, Li Manni L, Lecloux G, et al. Digital vs conventional workflow for one‑abutment one‑time immediate restoration in the esthetic zone: a randomized controlled trial. Int J Implant Dent. 2022;8:87. doi:10.1186/s40729-022-00406-6.
2. Garcia‑Torres F, Jurado CA, Rojas‑Rueda S, et al. Immediate implant therapy with full‑digital workflow to replace a central incisor. Dent J (Basel). 2025;13(2):73. doi:10.3390/dj13020073.
3. Pirooz P, Atri F, Gholami P, Bayat M. Digital implant placement accuracy: fully guided flapless single‑unit immediate‑loading protocol. Maxillofac Plast Reconstr Surg. 2023;45:19. doi:10.1186/s40902-023-00387-5.
4. Wang CW, Bhaskar V, Dickerman B, Kaigler D. Computer‑guided immediate implant placement with predigitally designed provisionalization: case report. Clin Adv Periodontics. 2018;8:39–44. doi:10.1902/cap.2017.170034.
5. Yilmaz H, Arınç H, Çakmak G, Atalay S, Dönmez MB, Yilmaz B. Effect of scan pattern on the scan accuracy of a combined healing abutment–scan‑body system (in vitro). J Prosthet Dent. 2022;S0022‑3913(22)00067‑1. doi:10.1016/j.prosdent.2022.01.018.
6. Çakmak G, Yilmaz H, Treviño Santos A, Kökat AM. Accuracy of different complete‑arch digital scanning techniques with a combined healing abutment–scan‑body system. ResearchGate preprint/PDF, 2021. (Conference award; methodology paper).
7. Kim GH, Park EJ, Cho YE. Comparison of scan data accuracy: implant scan body vs healing abutment used for scanning (in vitro). J Implantology and Applied Sciences. 2024;28(1):32–41. (Open access).
8. Chokaree P, Poovarodom P, Chaijareenont P, Rungsiyakull P. Customized vs prefabricated healing abutments in immediate sites: randomized controlled trial. J Clin Med. 2024;13(3):886. doi:10.3390/jcm13030886.
9. Ruhstorfer M, Güth JF, Stimmelmayr M, et al. Systematic review of peri‑implant conditions and aesthetic outcomes of customized vs conventional healing abutments. Int J Implant Dent. 2024;10:61. doi:10.1186/s40729-024-00581-8.
10. Enkling N, Marder M, Stoilov M, et al. Soft‑tissue response to different abutment materials (titanium, zirconia, veneered zirconia, PEEK): randomized human study. Clin Oral Implants Res. 2022;33(9):e281–e290. doi:10.1111/clr.13932.