





















Simultaneous implant-supported prosthetic rehabilitation, sinus lift and bone augmentation.

Dr. Nicolas JUNG
QUALIFIED SPECIALIST IN ORAL SURGERY
France
- Practising exclusively in oral surgery and periodontology
- Graduate of the Faculty of Lyon
- Les Aravis Clinic – Annecy
Case introduction:
A 60-year-old female patient presented at our office. She was in good health and a non-smoker, and had healthy periodontal tissue and good oral hygiene. Teeth 25, 26, and 27 had been missing for several years, and there was insufficient bone to place implants. However, quadrant four had been the priority, with 3 Axiom® REG implants being placed there in 2019. An inspection of quadrant three revealed significant damage to 36 and misalignment of 37.
Therefore, we opted for a shortened dental arch that would replace 25 and 26 but not 27. We decided to perform simultaneous sinus floor augmentation and implant placement, as there was only 4 mm of native bone at the implant sites.
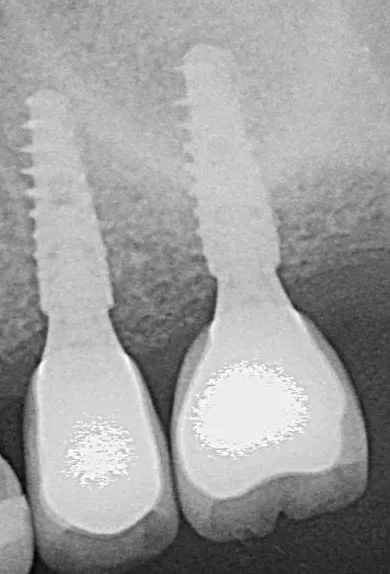
Initial situation
1-2. Panoramic radiography and cone-beam computed tomography showing vertical bone loss. With only 4 mm of sinus floor bone, implant placement was not feasible.


Surgical procedure:
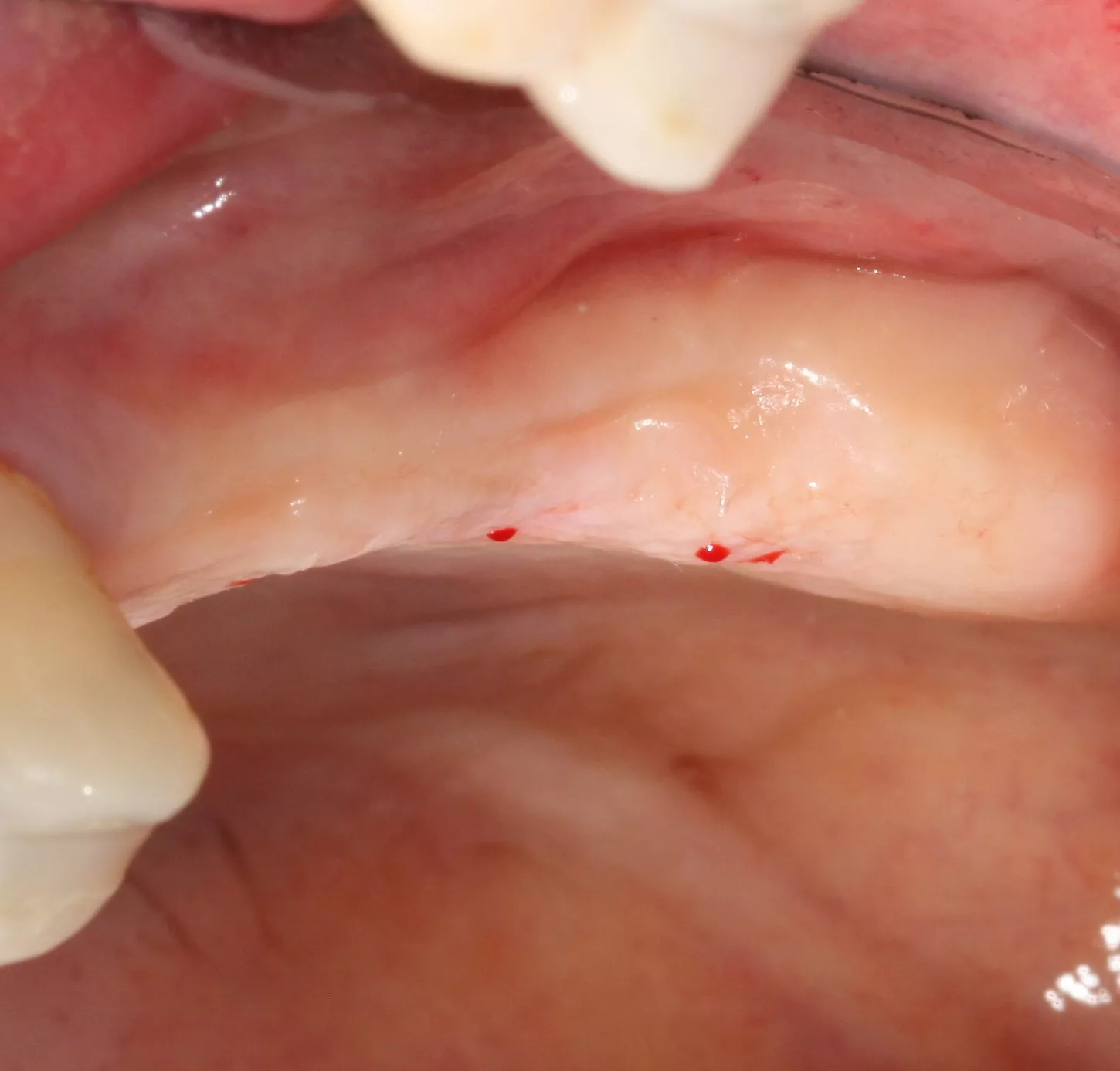
3a-b & 4a-b. Preoperative situation.
Free-end saddle. Periodontal tissue appeared healthy. Plenty of keratinized tissue. Notice the more extensive vestibular bone loss around 25.

3a

4a

3b
4b
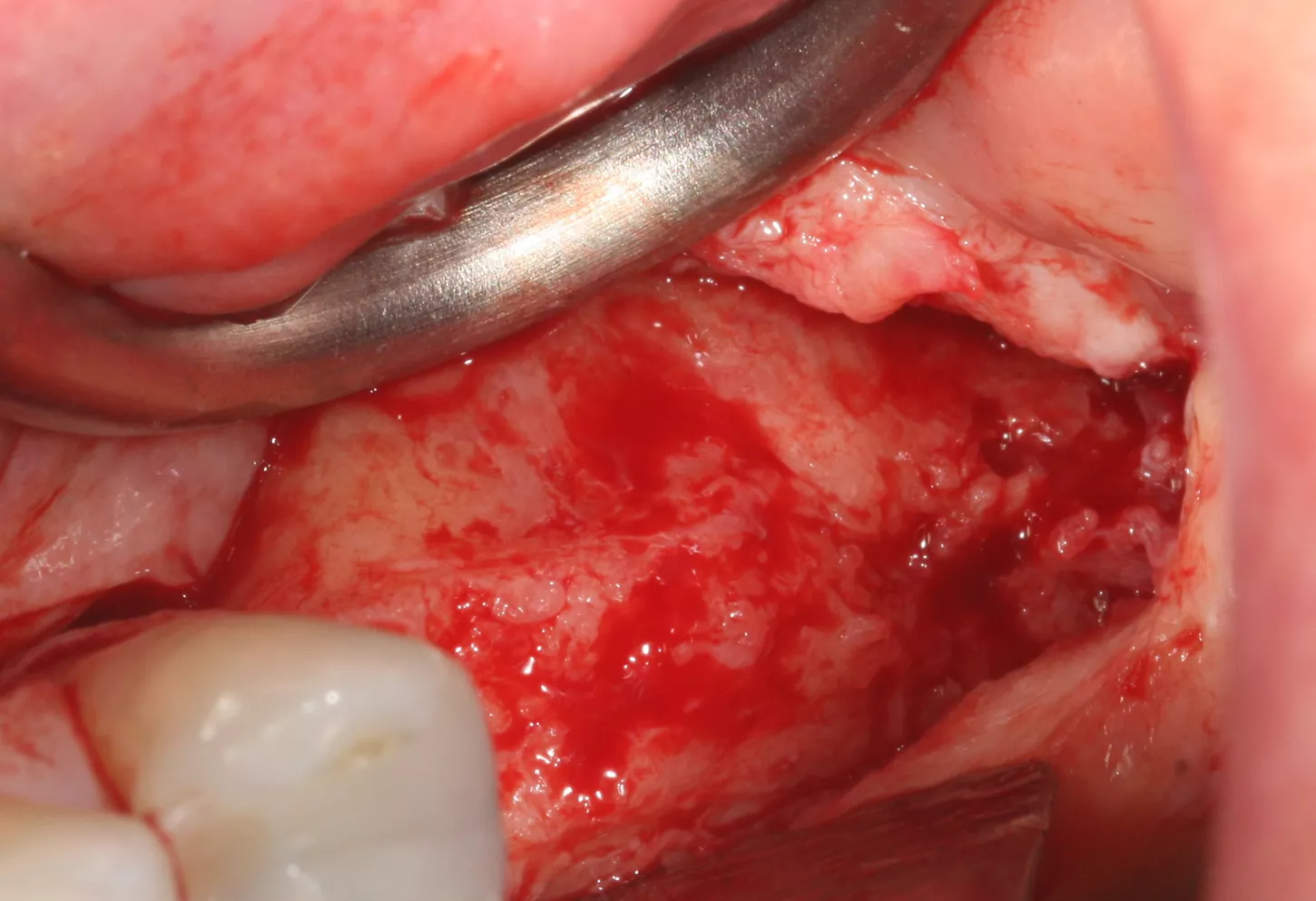
5. A full-thickness flap was elevated and a releasing incision made mesial to 24. Care must be taken at this stage not to damage the periosteum.
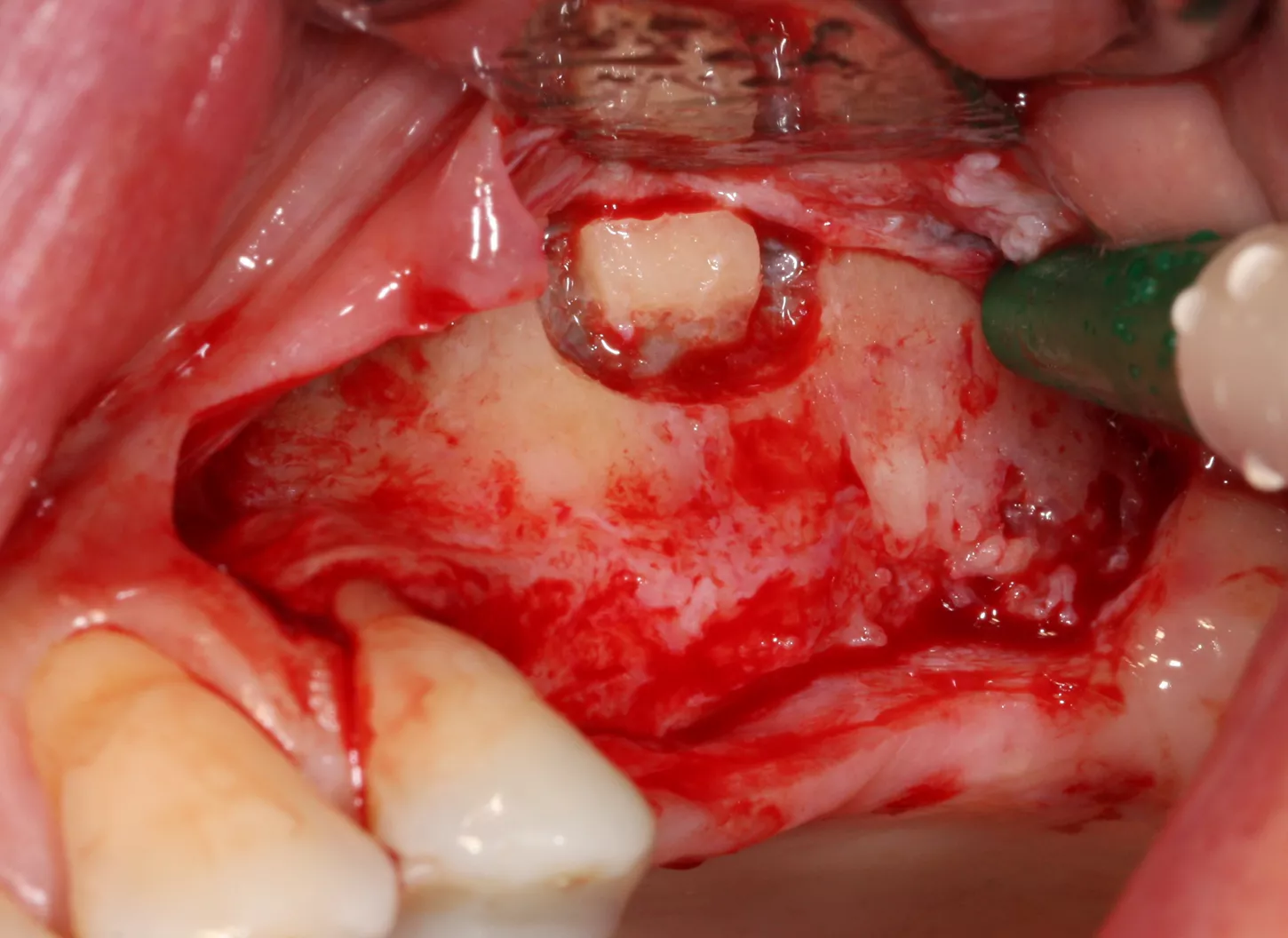
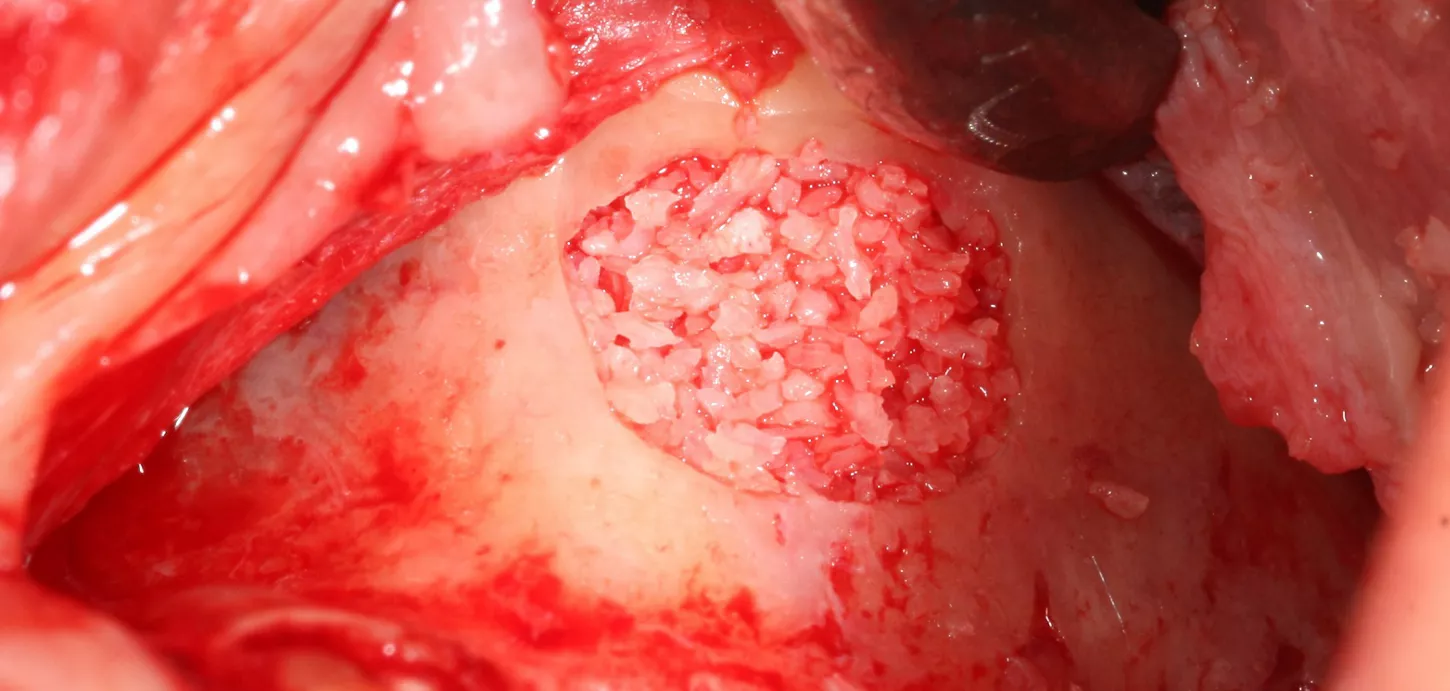
6. A lateral sinus lift was performed by creating a 7 × 5 mm window using a round tungsten carbide bur followed by a diamond bur.
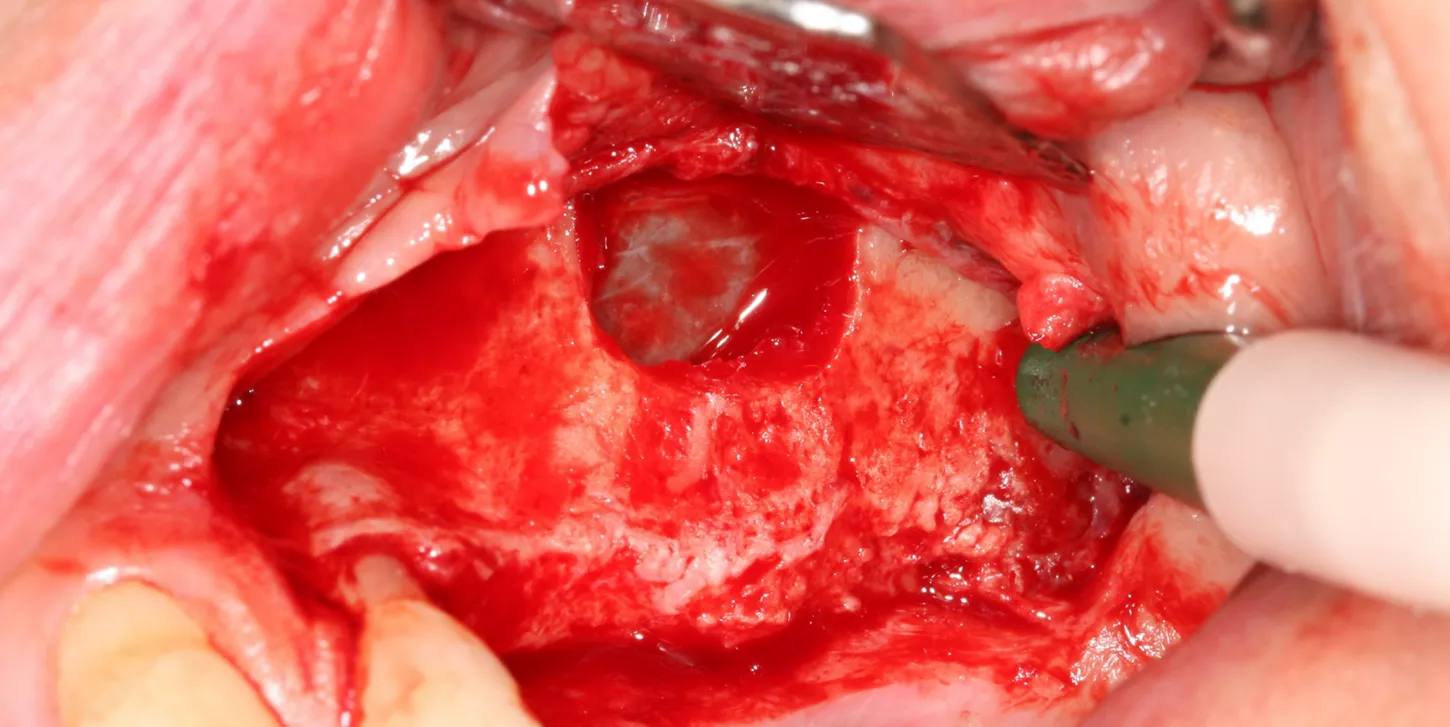
7. The bony window was removed and placed in saline solution so that it could be placed back in position after grafting. The Schneiderian membrane was released without perforation.
8. The sinus was elevated with cortical/cancellous allograft of a particle size of 0.5 mm and volume of 1.5 cc.
Prosthetic restoration:
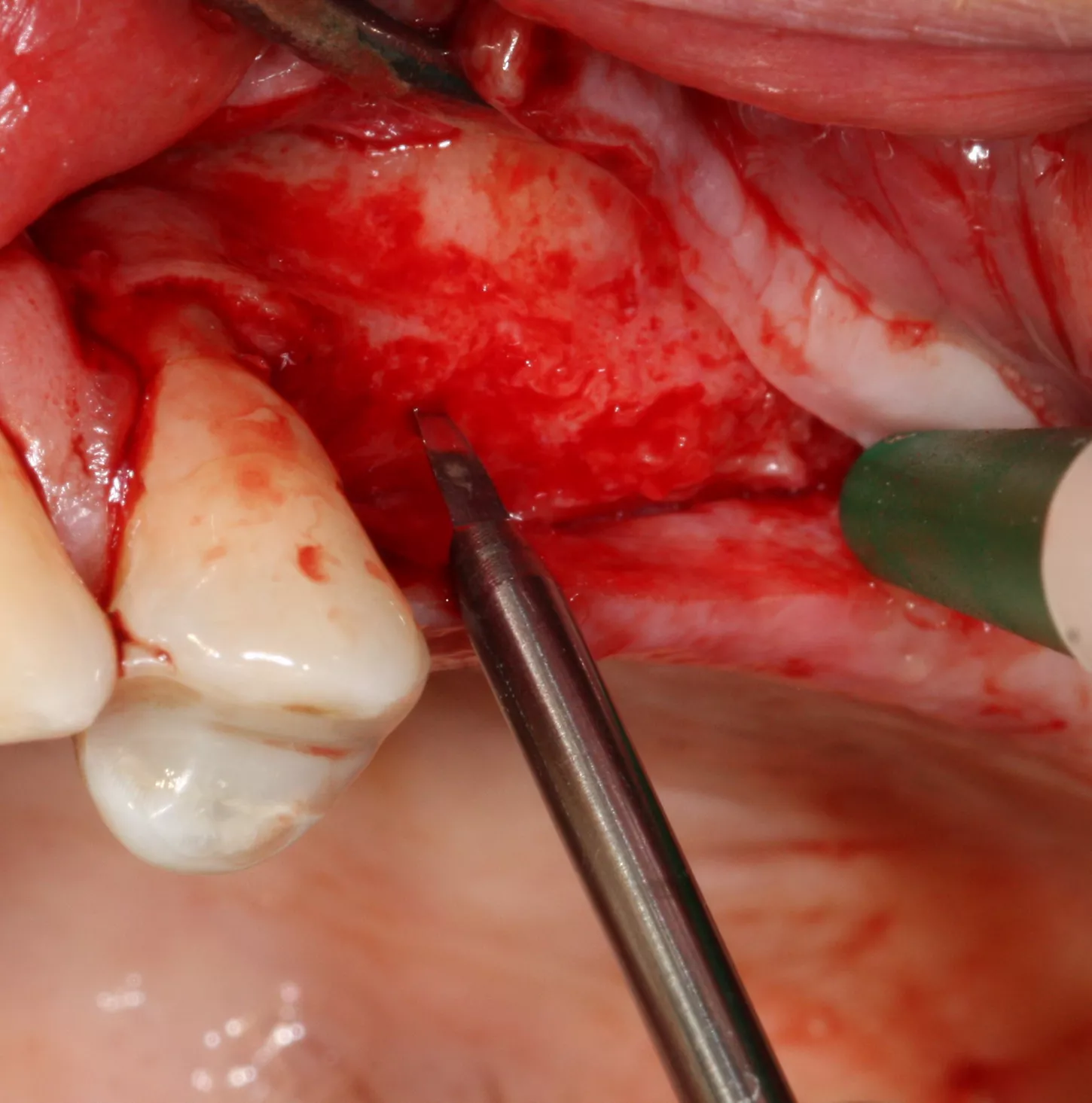
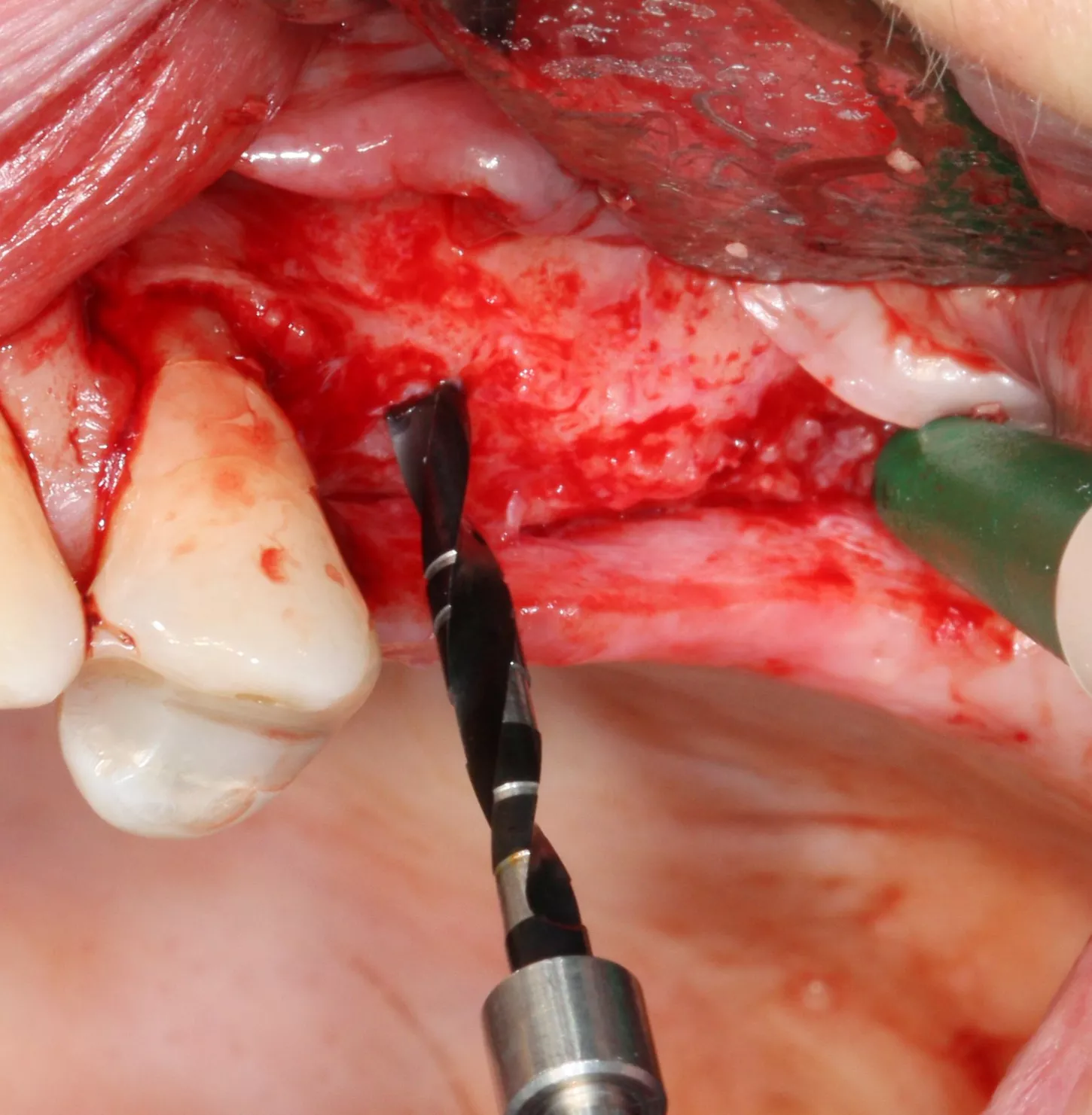
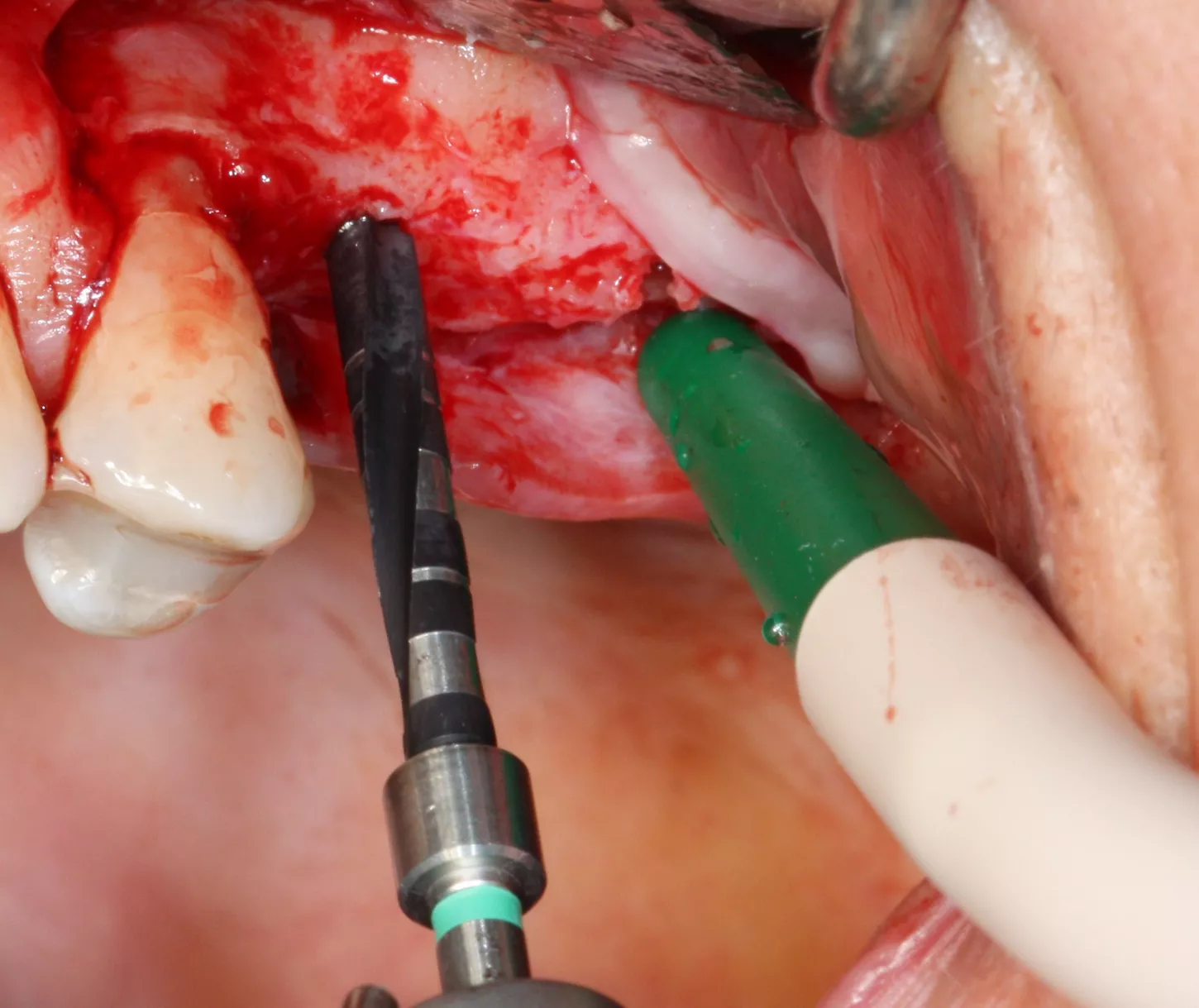
9-10-11. The patient had D3 bone density. Hence an undersized drilling protocol was employed, the final drill diameter being one less than that of the implant. The green drill was used for the 25 implant (diameter 3.4) and the red one for the 26 (diameter 4.0).
9
10
11
12a-b-c. The design of the Axiom X3® ensures atraumatic implant placement with the micro motor. The Axiom X3® also preserves bone, even if the ridge is thin and resorbed. Despite the meager quantity of vestibular cortical bone, there was no perforation or rupture of the crestal margin.


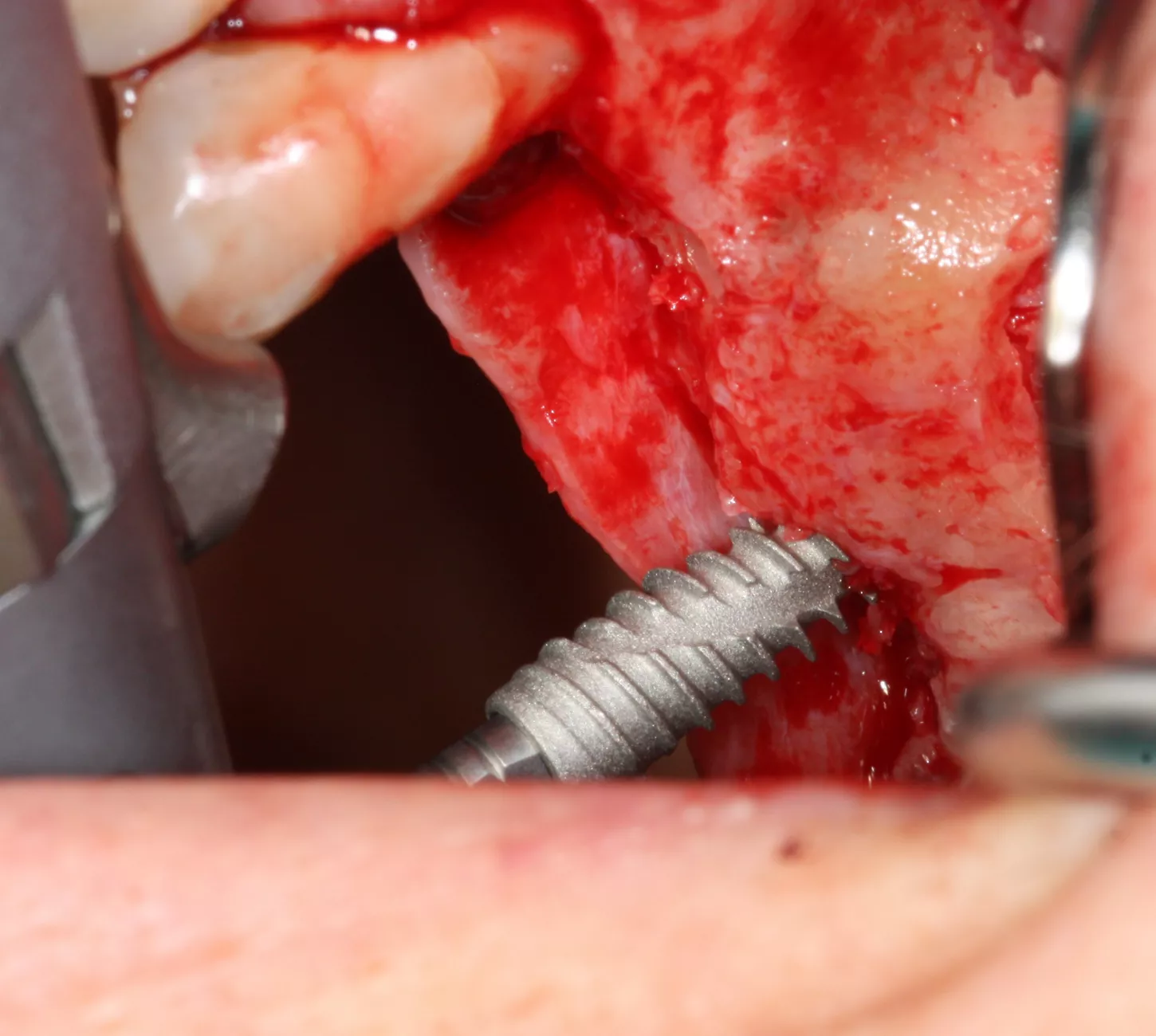
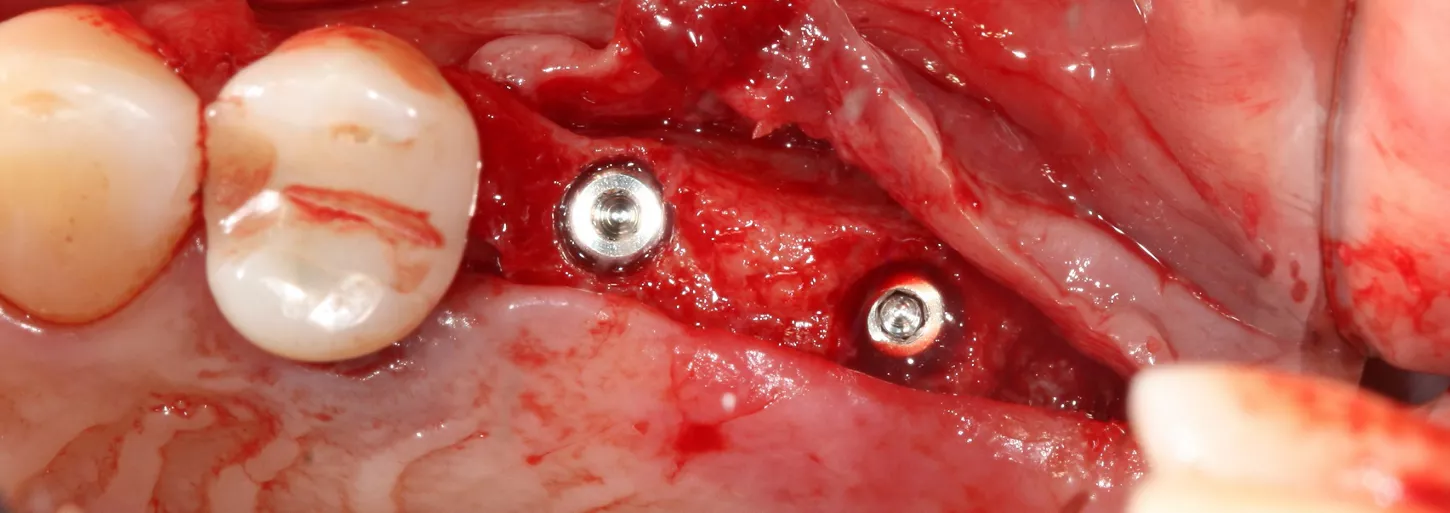
13. The implants were placed 0.5–1 mm subcrestally. Note the thinness of the vestibular cortical bone at the 25 implant on this occlusal view. Despite this, we achieved perfectly acceptable stability values of 19 and 20 Ncm.
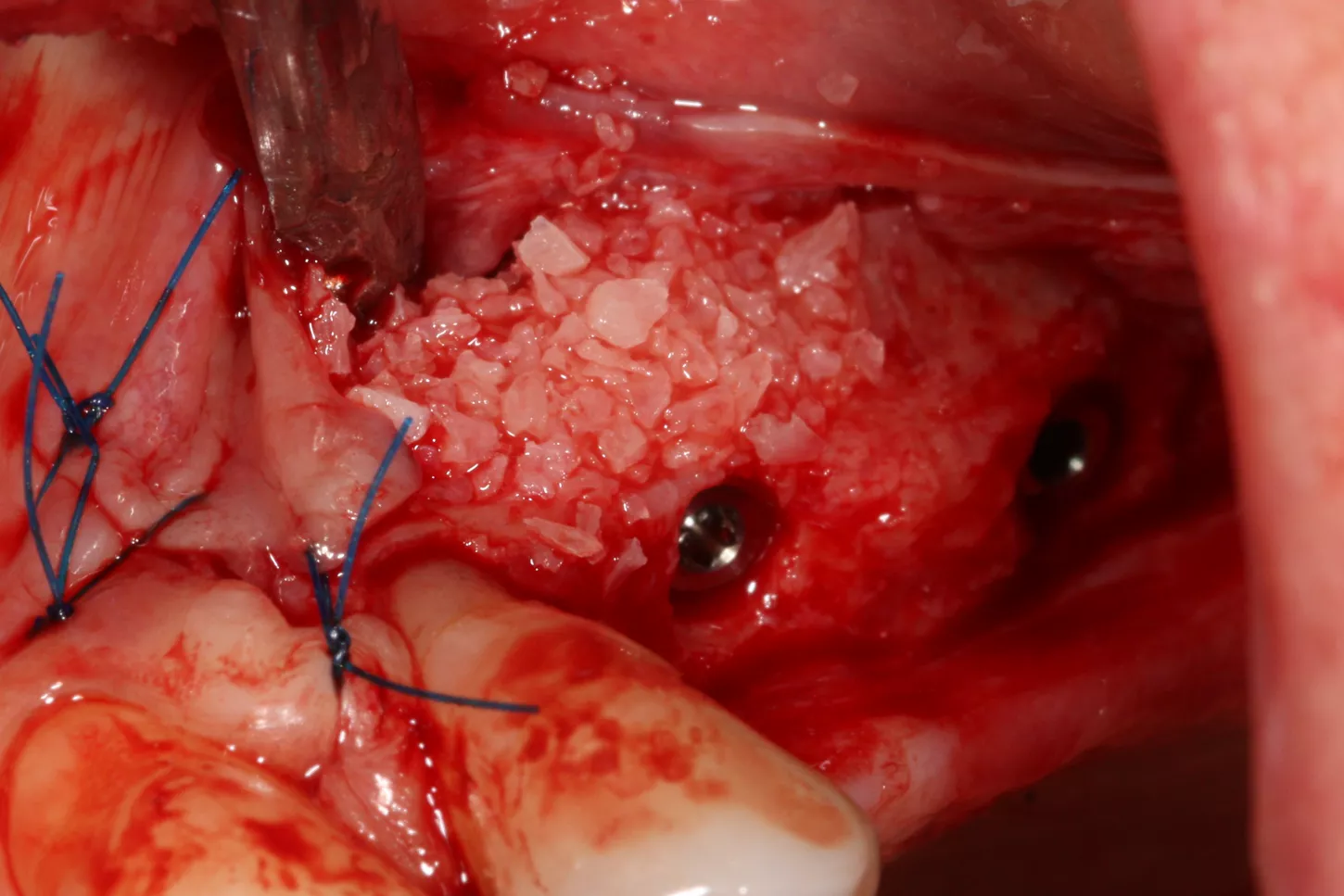
14. Graft material added to the vestibular aspect of 25 to offset the bone loss and ensure long-term implant survival.
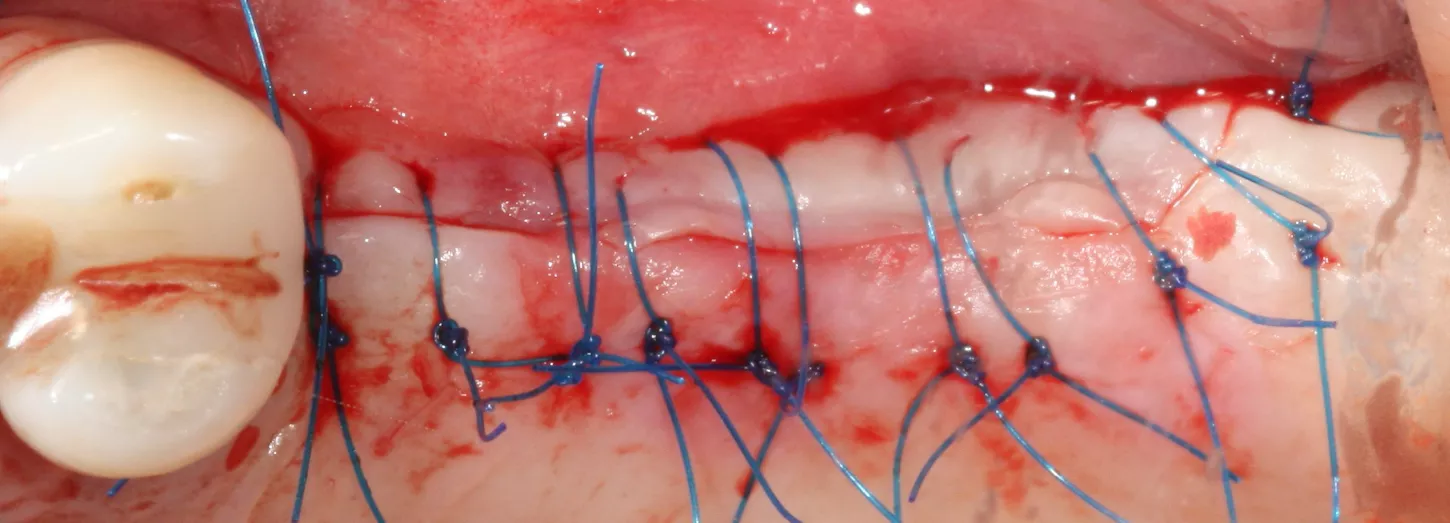
15. The surgical site was closed with 5/0 non-absorbable monofilament polypropylene sutures, removed 10 days postoperatively. The implants were buried with their closure screws.
Prosthetic restoration:
16. Postoperative panoramic radiograph.

Final situation:
18. 3 years follow up panoramic radiograph.
17. Two single-unit zirconia-veneered Simeda® crowns were fabricated on titanium bases.

19. Final prosthesis in the mouth 3 years post implant placement.

Conclusion :
In this case, the Axiom X3® implants gave us better control of insertion into the patient’s native bone and ensured good primary stability despite the bone graft. The drilling protocol was adapted to the patient, with the final drill being omitted due to her D3 bone density. The implant’s atraumatic apex made placement in the bone graft safe, affording us greater peace of mind in an area where visualization of the surgical field is limited.