





















Digital Prosthetic Workflow Efficiency and Guided Soft Tissue Healing Around Dental Implants: A Case Study Comparing HealFit® SH and Conventional Healing Abutments.

Dr. Karim RACHIDI
Qualified Specialist in Oral Surgery
Manchester, United Kingdom
- Qualified Specialist in Periodontology and Implant Dentistry
- Postgraduate Diploma (DESS) in Periodontology and Dental Implants
- Expert in full-arch implant rehabilitation and digital implant workflows
- Clinical Lead and Principal Dentist at Synergy Leyland private practice in the United Kingdom
Case introduction
A 64-year-old male patient, in good general health, presented to our clinic with partial edentulism associated with compromised aesthetics, and impaired masticatory function. The patient expressed dissatisfaction with his smile and reported difficulty chewing due to multiple missing teeth.
Clinical and radiographic findings revealed missing teeth, failing prosthetic restorations, and chronic odontogenic infections, collectively contributing to functional impairment which negatively impacted the patient’s self-esteem and overall well-being, leading them to seek comprehensive implant-based rehabilitation. Given the patient’s clinical presentation and functional needs, a digitally driven rehabilitation pathway was selected to leverage the efficiency and predictability of current digital implant ecosystems. Contemporary digital workflows provide improved diagnostic accuracy, streamlined communication, and more predictable restorative outcomes compared with analogue approaches [1]. The integration of virtual planning, CAD/CAM‑guided surgery, and scannable anatomical healing abutments aligns with evidence demonstrating enhanced precision, reduced technique sensitivity, and better intraoral scanning fidelity in implant‑supported rehabilitation. Collectively, these advancements made the digital pathway the most seamless and biologically favourable treatment choice for this case [2].
Treatment planning
- Periodontal stabilisation was first carried out to establish a healthy soft‑tissue environment prior to restorative and implant therapy. The esthetic rehabilitation plan included implant placement in sites LR6, LL5, LL6, and UL4, combined with porcelain veneers and crowns from UR3 to UL3 to harmonize the maxillary anterior smile.
- Edentulous sites were scheduled for implant-supported crowns. Axiom X3® Bone Level implants were selected based on their ability to achieve optimal primary stability and prosthetically driven positioning.
- A fully digital workflow was employed, progressing from digital smile design to virtual planning of implant positions, surgical guide fabrication, and including the digital selection and placement of HealFit® SH abutments and the corresponding implants.
Initial situation
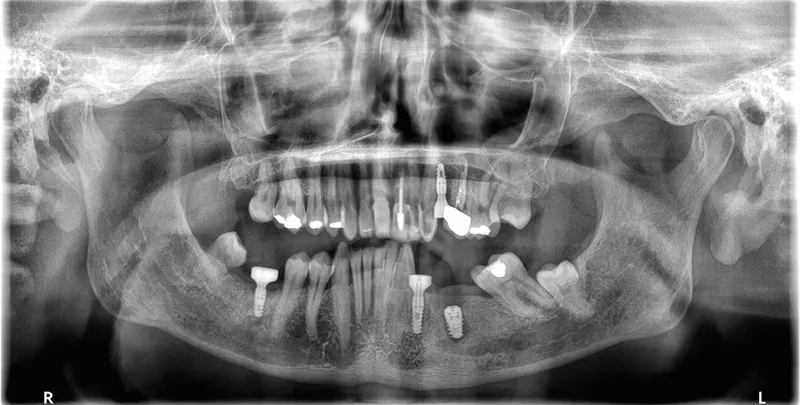
1. Panoramic view showing severe bone loss around tooth 15, confirming hopeless prognosis.

1
2a. 2b. Preoperative frontal and occlusal view of the lower arch showing multiple missing teeth.

2a

2b
3a. 3b. Implant and Healfit® SH planning in coDiagnostiX®.Digital smile design illustrating esthetic outcome using Smilecloud®.

3a

3b
4. Tooth‑supported implant surgical guides for implant placement on position LR6 LL4 LL5 and UL4.

4
A preliminary digital smile design was generated to support the esthetic assessment and facilitate discussion of treatment objectives. This rapid visual simulation enabled the patient to preview the anticipated anterior maxillary outcome, improving comprehension of the proposed plan and helping align expectations with realistic treatment results. This step enhanced patient engagement and supported informed decision‑making at the outset of care.
Surgical procedure
Although the case was digitally planned and guided, this does not require a flapless approach. Flap elevation remains appropriate when bone quality is uncertain, augmentation is needed, or direct visualization is necessary. Evidence shows that guided surgery improves accuracy whether performed with or without a flap, and flapless protocols may reduce deviation and surgical time [3]. However, sites with compromised bone often benefit from open‑flap access, confirming that fully guided surgery can still be combined with flap elevation when clinically indicated [2, 4].
5a. 5b. Digitally guided osteotomy and implant placement on LL4 (Lower LEFT 4) and LL5 (Lower LEFT 5) 0.5mm sub-crestal performed using the Integral Kit, following the manufacturer’s drilling sequence and implant placement protocol after flap elevation.

5a

5b
6a. 6b. Axiom®X3 implants used in this case (Ø 4 mm × 10 mm) and Ø 4.6 mm × 8 mm.

6a

6b
In the posterior left mandible, bone conditions varied across sites and dictated different healing protocols. At LL5, the initial panoramic radiograph showed evidence of a previous extensive infection, resulting in compromised bone quality. Despite under‑preparing the osteotomy to improve implant engagement, adequate primary stability could not be achieved; therefore, the implant was placed subcrestally and covered to allow undisturbed osseointegration under a submerged healing protocol.
In contrast, the adjacent LL4 site presented more favorable bone conditions and achieved high primary stability at placement, enabling immediate placement of a HealFit® anatomical healing abutment to establish transmucosal shaping from surgery. After 3 months, osseointegration was satisfactory at both sites, though soft‑tissue maturation was notably superior at LL4, consistent with early guided soft‑tissue contouring.
Similarly, at LL6 the implant exhibited insufficient primary stability (< 20 N·cm) and was placed subcrestally with a cover screw for submerged healing, while the mesial implant at LL5 (when stability was adequate > 45 N·cm) received a HealFit® abutment to support soft‑tissue maturation during healing (7.).
7. Distal implant placed with a cover screw, and mesial implant restored with a HealFit® SH anatomical healing abutment.

7
Suturing was adapted to each implant site. The distal implant was fully submerged with a cover screw, requiring complete primary closure. At the mesial implant, where a HealFit® SH abutment was placed, only two simple interrupted sutures were placed mesially and distally to stabilize the soft tissues.
8. Suturing was adapted to each implant site. The distal implant was fully submerged with a cover screw, requiring complete primary closure. At the mesial implant, where a HealFit® SH abutment was placed, only two simple interrupted sutures were placed mesially and distally to stabilize the soft tissues.

8
Three months after implant placement, a second‑stage surgery was performed at the distal site to uncover the implant following successful osseointegration. A standard healing abutment was placed, as this implant had initially been placed subcrestally with a cover screw due to insufficient primary stability and required conventional freehand placement.
In contrast, the mesial implant had achieved adequate primary stability at surgery, allowing the use of a HealFit® SH anatomical healing abutment from the time of placement. This resulted in progressive transmucosal shaping without the need for additional surgical intervention. At re‑evaluation (8.), peri‑implant soft‑tissue maturation was already complete at this site, illustrating the clinical advantages of immediate transmucosal conditioning, including reduced need for second‑stage surgery, minimised soft‑tissue trauma, improved emergence profile development, and a more streamlined prosthetic workflow.
9. Panoramic radiograph taken on the day of implant placement.
9
10. Periapical radiograph taken on day 3 post surgery showing the implant with the HealFit® SH healing abutment in position.

10
For the maxillary single‑tooth implant, a fully digital guided workflow was used, allowing a flapless approach. Soft‑tissue access was achieved with a tissue punch through the surgical guide [5], followed by osteotomy preparation using the Axiom® X3 drilling protocol. The implant achieved high primary stability (≈50 N·cm), enabling immediate placement of a HealFit® SH without suturing.
11a. 11b. 11c. 11d. Flapless guided placement of the maxillary implant with tissue‑punch access, Axiom X3 osteotomy, and immediate HealFit® SH placement without sutures.

11a

11b

11c

11d

Healfit® SH for optimal tissue shaping?
A 3‑in‑1 solution that preserves the biological seal and recreates a natural emergence profile thanks to its 5 anatomical shapes.
Clinical outcome
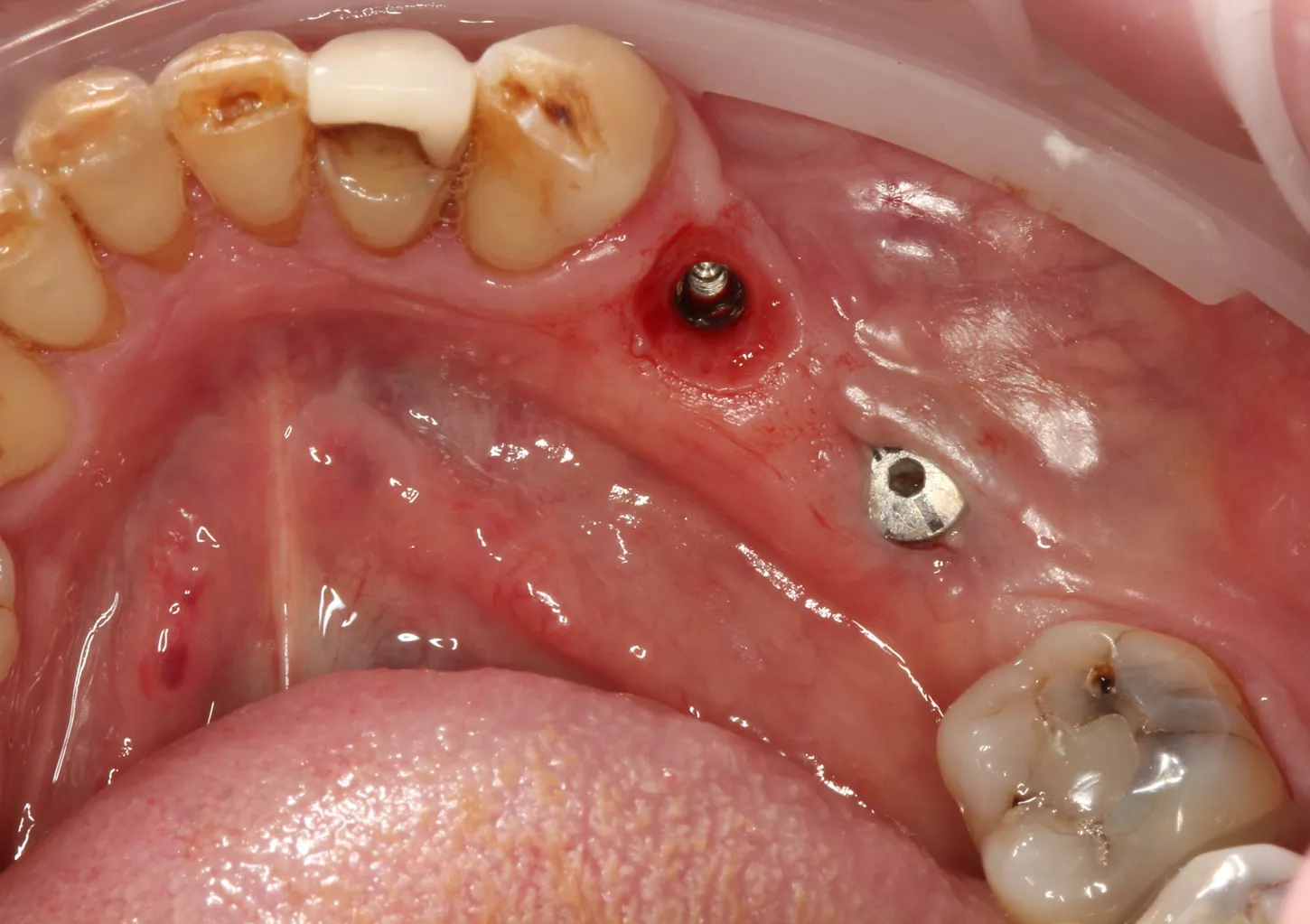
Soft‑tissue healing differed notably between the two sites. The mesial implant restored with a HealFit® SH abutment showed thicker, well‑adapted peri‑implant mucosa with minimal erythema inflammation and a stable, guided emergence profile, reducing the need for secondary tissue conditioning. In contrast, the distal implant with a traditional healing abutment demonstrated localized redness, a compressed circular healing pattern, and no guidance of soft‑tissue contour, features commonly associated with conventional implant exposure techniques, which can produce increased soft‑tissue reactivity and later need for tissue shaping.
12a. 12b. 12c. 12d. 12e. Soft‑tissue healing comparison: HealFit® SH shows anatomic, well‑shaped mucosa, while the conventional healing screw displays a flat, compressed circular pattern.

12a

12b
12c

12d

12d
Prosthetic restoration
The prosthetic plan consisted of restoring the site with a screw‑retained single implant crown using an X‑Base® abutment and a zirconia screw‑retained restoration. A screw‑retained design was selected due to its well‑recognized advantages over cement‑retained options, including predictable retrievability, elimination of excess cement and reduced peri‑implant inflammation risk, superior marginal control, and a fully reversible prosthetic workflow.
13a. 13b. 13c. The intraoral scan was processed to generate a 3D digital model for prosthetic design.

13a

13b

13c
14a. 14b. 14c. 14d. 14e. Exocad® prosthetic design based on the intraoral scan and implant position.

14a

13b

14c

14d

14e
15a. 15b. 15c. 15d. The screw retained monolithic zirconia crowns were milled and bonded to Anthogyr X-Base® abutments.

15a

15b

15c

15d
The prosthetic plan consisted of restoring the site with a screw‑retained single implant crown using an X‑Base® abutment and a zirconia screw‑retained restoration. A screw‑retained design was selected due to its well‑recognized advantages over cement‑retained options, including predictable retrievability, elimination of excess cement and reduced peri‑implant inflammation risk, superior marginal control, and a fully reversible prosthetic workflow.
16a. 16b. 16c. 16d. Passive fit of the screw‑retained crown confirmed clinically, the access sealed with PTFE and composite.

16a

16b
16c
17a. 17b. Periapical radiograph of the implant at tooth position (LL5 LL4 and UL4 and), obtained 4 months post‑implantation

17a
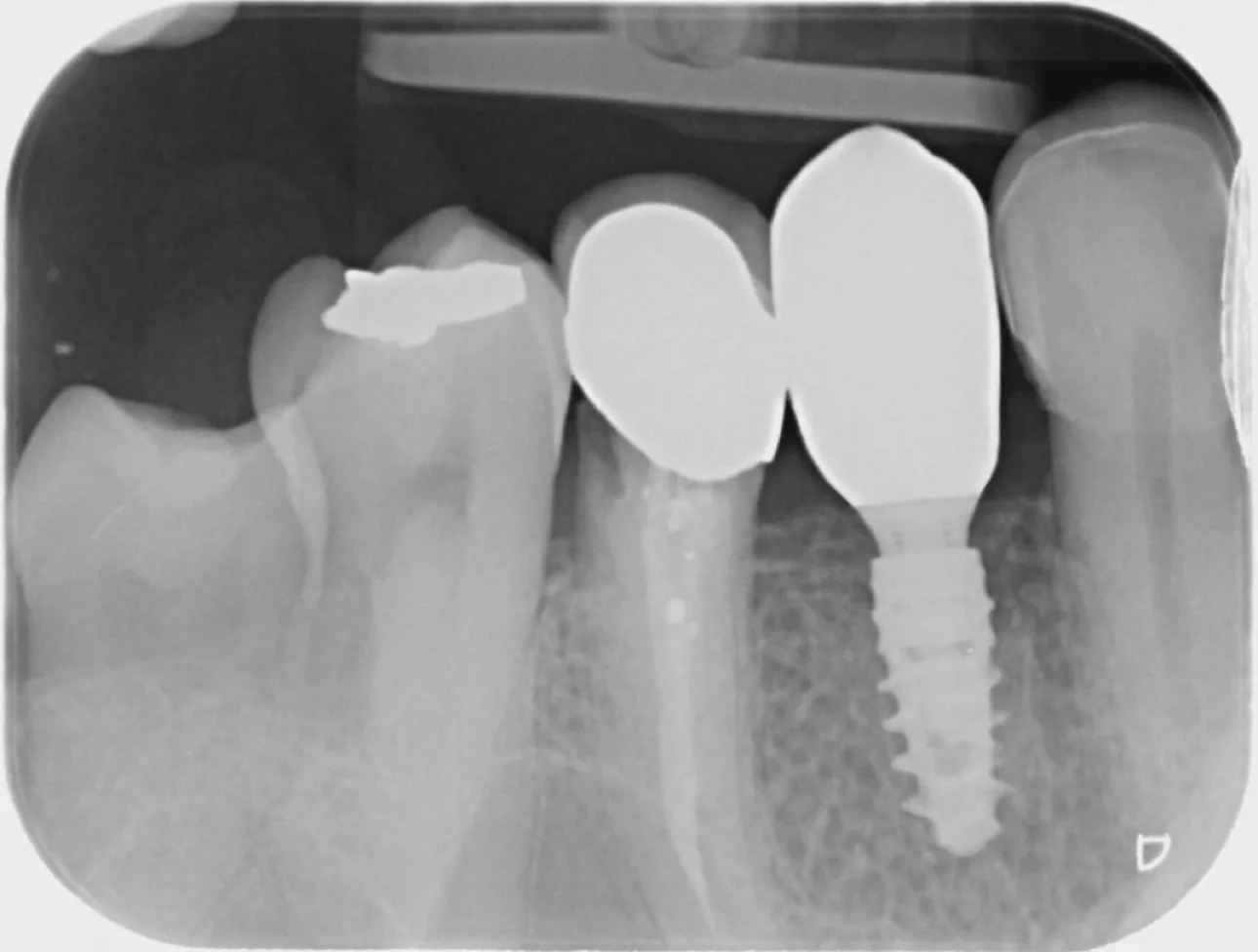
17b
18. Final smile.

18
Conclusion
This case highlights how a digitally integrated workflow and implantology ecosystem supports site‑specific adaptation, allowing the clinician to combine flapless access, soft‑tissue punch, and flap elevation within one coherent plan. Digital guidance enabled minimally invasive approaches where appropriate, reducing postoperative discomfort and simplifying soft‑tissue handling.
A clear distinction was observed between the sites restored with an anatomical HealFit® SH healing abutment, which developed a natural emergence profile without additional soft‑tissue conditioning, and the site managed with a conventional healing screw, which required a second‑stage procedure and longer maturation. This difference translated into shorter chair time and fewer interventions for the HealFit® SH site. Overall, the case demonstrates how the Axiom® ecosystem supports flexible surgical choices while maintaining a streamlined and predictable prosthetic pathway.
References
1. Clark J. The Role of Digital Technologies in Immediate Prosthetic Rehabilitation Post-Implant Placement. 2025.
2. 1 RP, 1 RK, Chandak2 A, Deshmukh2 S, Banerjee2 R. Fully Digital Workflow For Implant-Supported Prosthetic Rehabilitation: A Case Report. International Journal of Research and Analytical Reviews (IJRAR) 2023.
3. Subramani K. Is computer-guided implant placement with aflapless approach more accurate than with a flapped surgical approach? Evidence-Based Dentistry 2022.
4. Sheth K. Evaluation of biological tissue outcomes around implants placed in a flapless manner versus a flapped manner: learning from the literature. ITI Blog 2023.
5. Rajaram V, Dedhia DK, Mahendra J, Parameswari D, Khanna S. Flapless soft tissue punch technique for implant placement- A case report. International Journal of Oral Health Dentistry 2020. 6(3): pp. 232–235.