





















3D posterior mandibular reconstruction using autogenous split bone block technique and implantation using Axiom X3®.

Dr. Franck AFOTA
QUALIFIED SPECIALIST IN ORAL SURGERY
France
- Former Intern and Specialist Assistant at Nice Hospitals.
- Attached practitioner and lecturer in the Oral and Maxillofacial Surgery department of Nice University Hospital - Institut Universitaire de la Face et du Cou.
- Scientific Co-Director of the University Diploma in Pre-implant Bone Surgery (DU COPI), IUFC, CHU NICE.
Case introduction:
A 38-year-old patient presents for oral surgery consultation referred by her dentist for the replacement of teeth 35 and 36. The patient is in good health, a smoker at the time of the consultation, with the will to quit. The initial CT scan shows significant bone atrophy in all three spatial directions (height 4 mm above the mental foramen, Cawood 5) with a low well-rounded ridge presentation [1]. The prosthetic project was to create two implant-supported crowns at sites 35 and 36. To regenerate the bone at the site, we opted for an autogenous bone graft protocol as described by Professor F. Khoury. The aim is to reconstruct the bone volume of the site in the horizontal and vertical directions with a high tolerance [2].
Autogenous bone grafts involve taking bone from the patient himself, generally from the mandible, chin or iliac crest, and transplanting it into the deficient area. This technique has several significant advantages over other methods of bone regeneration, such as the use of allografts, xenografts or synthetic biomaterials. Unlike bone substitute materials, autogenous grafting is osteogenic, thus ensuring better integration and faster and more effective bone regeneration. Autogenous bone also has intrinsic osteoinductive and osteoconductive properties, promoting the growth and differentiation of bone cells [3].
Biologically speaking, autogenous bone contains living cells and growth factors that accelerate the healing and bone regeneration process. These exceptional biological characteristics not only enable optimal integration of the graft, but also long-term stability of the dental implants.
Furthermore, the economic aspect of autogenous grafting is a significant advantage. Compared to other techniques requiring the use of expensive biomaterials or grafts from tissue banks, autogenous grafting, although surgically more complex, is often a less expensive option for patients. The immediate availability of the graft material also reduces treatment times, facilitating faster and more efficient care [3-5].
Treatment plan:
Bone was taken from the mandibular ramus, providing enough blocks for defects up to three teeth wide. It is preferred for horizontal or vertical augmentation and unilateral sinus augmentation [3]. Harvesting and grafting occurred in one surgery. Two Axiom X3® implants were placed 5 months after bone regeneration, followed by a connective epithelial graft 3 months later.
Initial situation:
1. Cawood 5 mandibular atrophy in the posterior mandibular sector with absence of teeth 35 36.

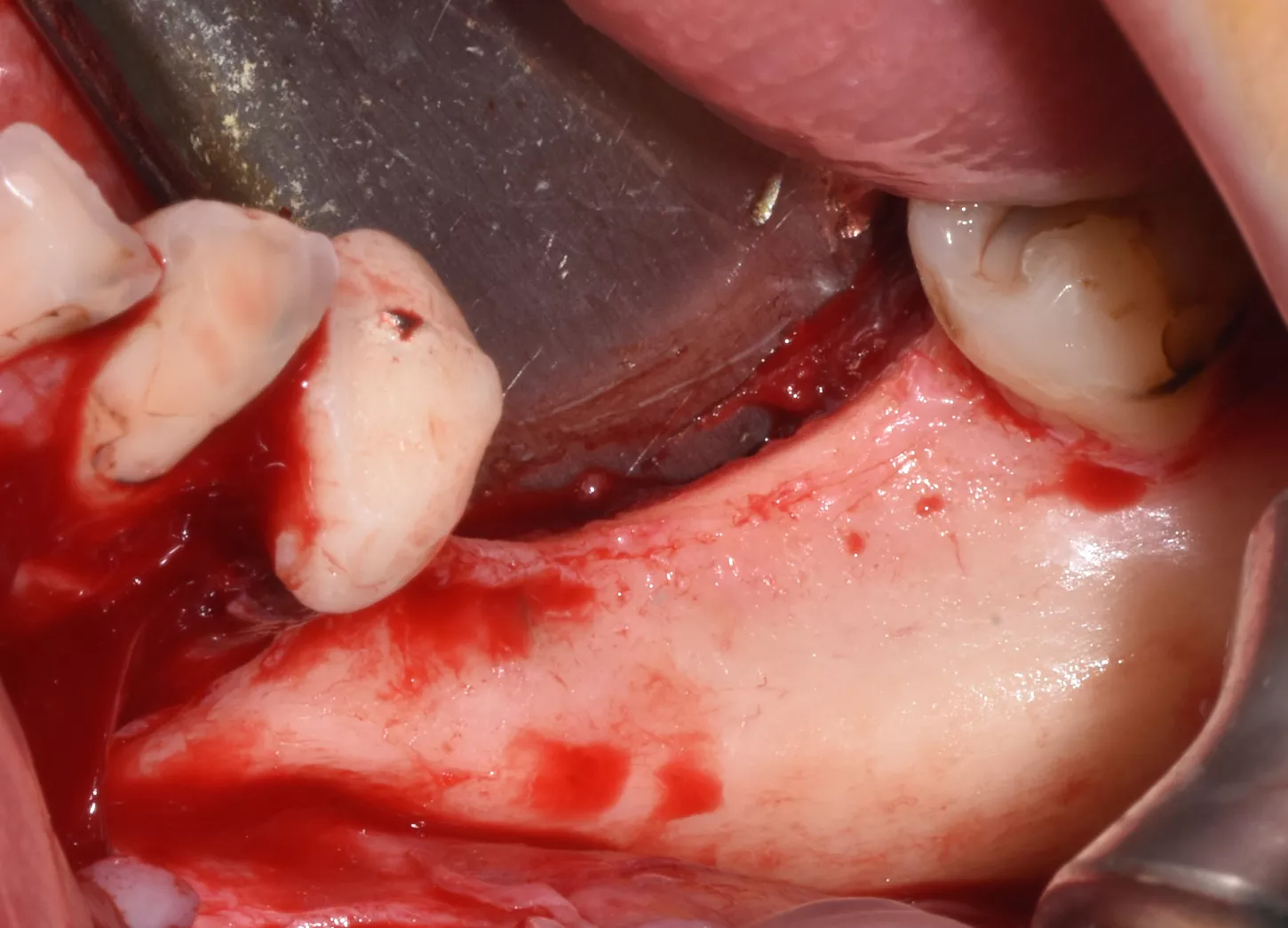
Surgical procedure:
2. Incision and detachment of anatomical structures, highlighting of the inferior dental nerve at the level of its emergence from the mental foramen. 3D bone atrophy is noted. Tissue relaxation is achieved by periosteal incisions in order to release tension and close the site properly.
3 . Split bone block technique using autogenous cortical plates taken from the left ramus according to F. Khoury's protocol.
One buccal plate and one lingual plate are positioned and osteosynthesised with 1 mm Stoma screws.
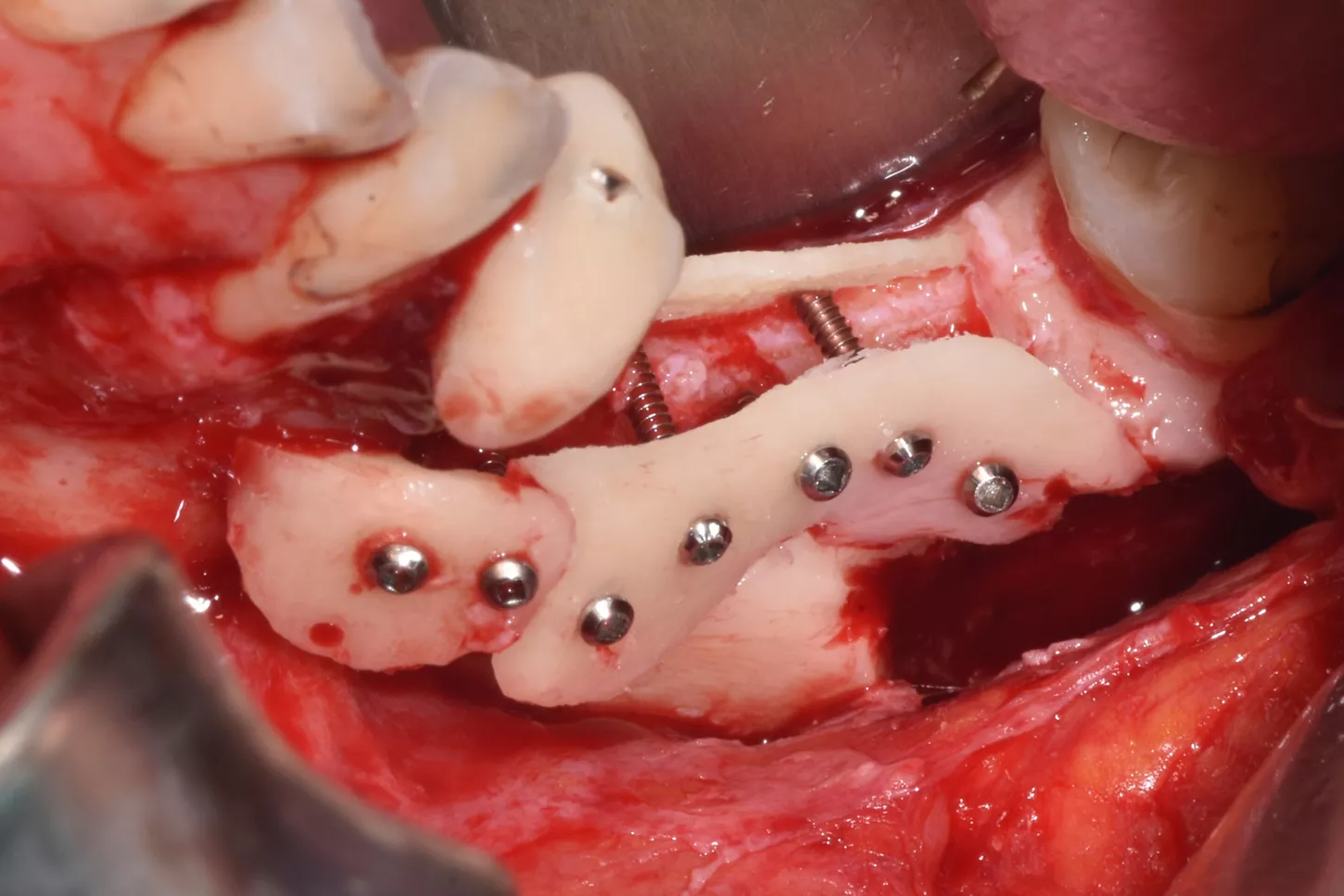
4. Forming and filling the gap with a mixture of autogenous/xenogeneic bone mixed with PRF (sticky bone).

5. Five months later, the site was reopened and two Axiom X3® Ø4 x 10 mm implants were placed in positions 35 and 36. The implants were positioned infra-crestally using the submerged technique with a torque of 25 Ncm.
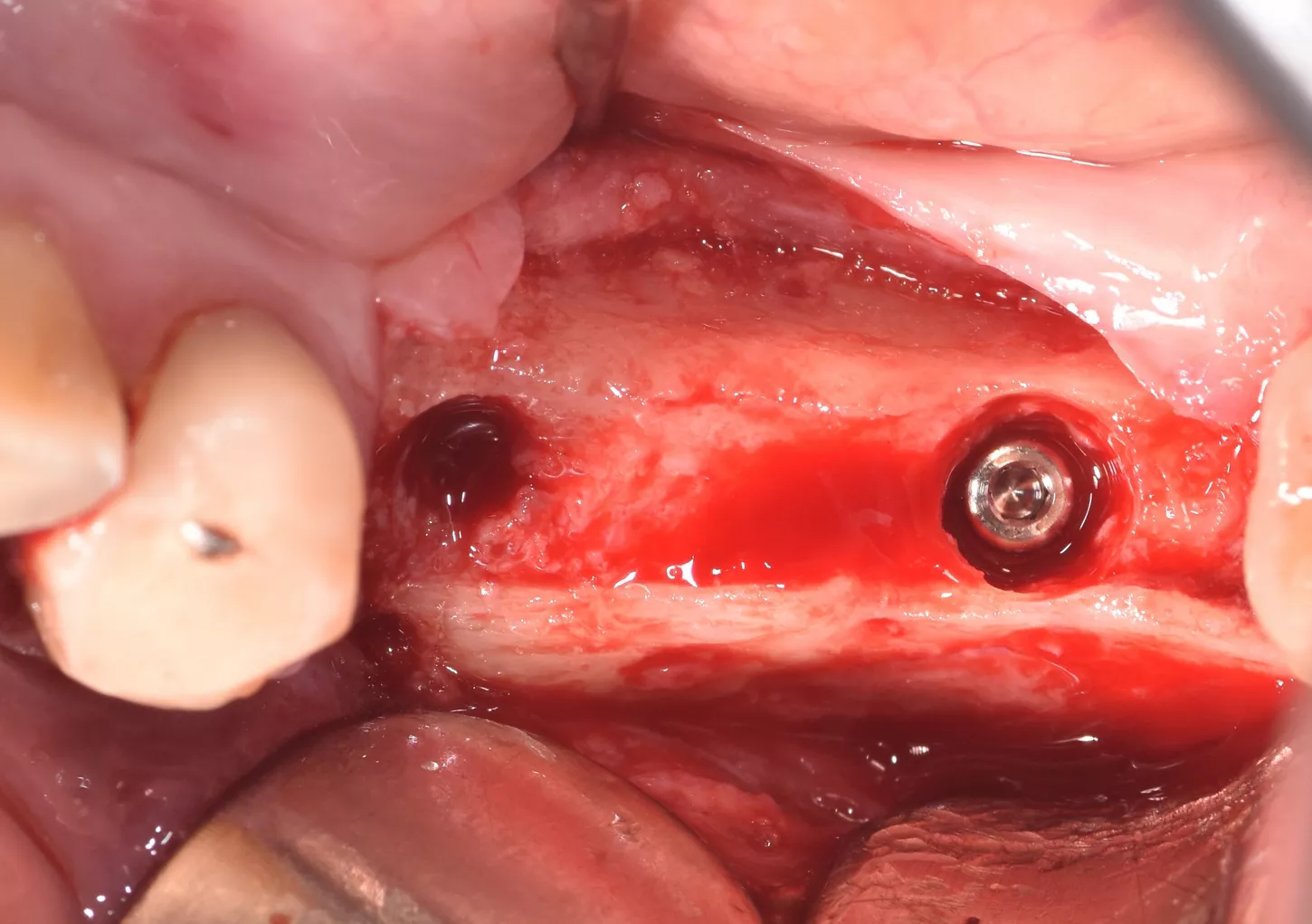
6 . Infra crestal position of the implants in the fully regenerated bone.

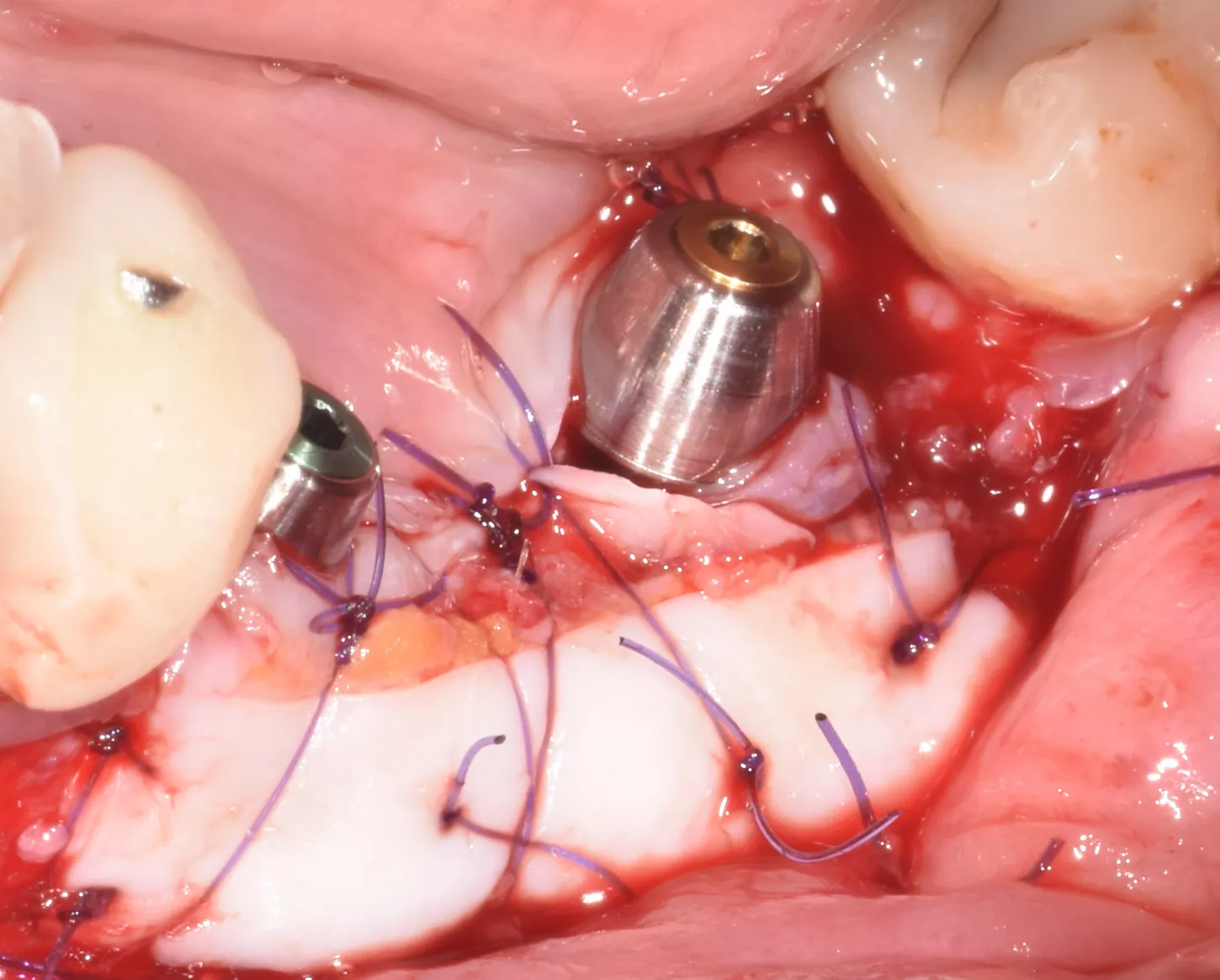
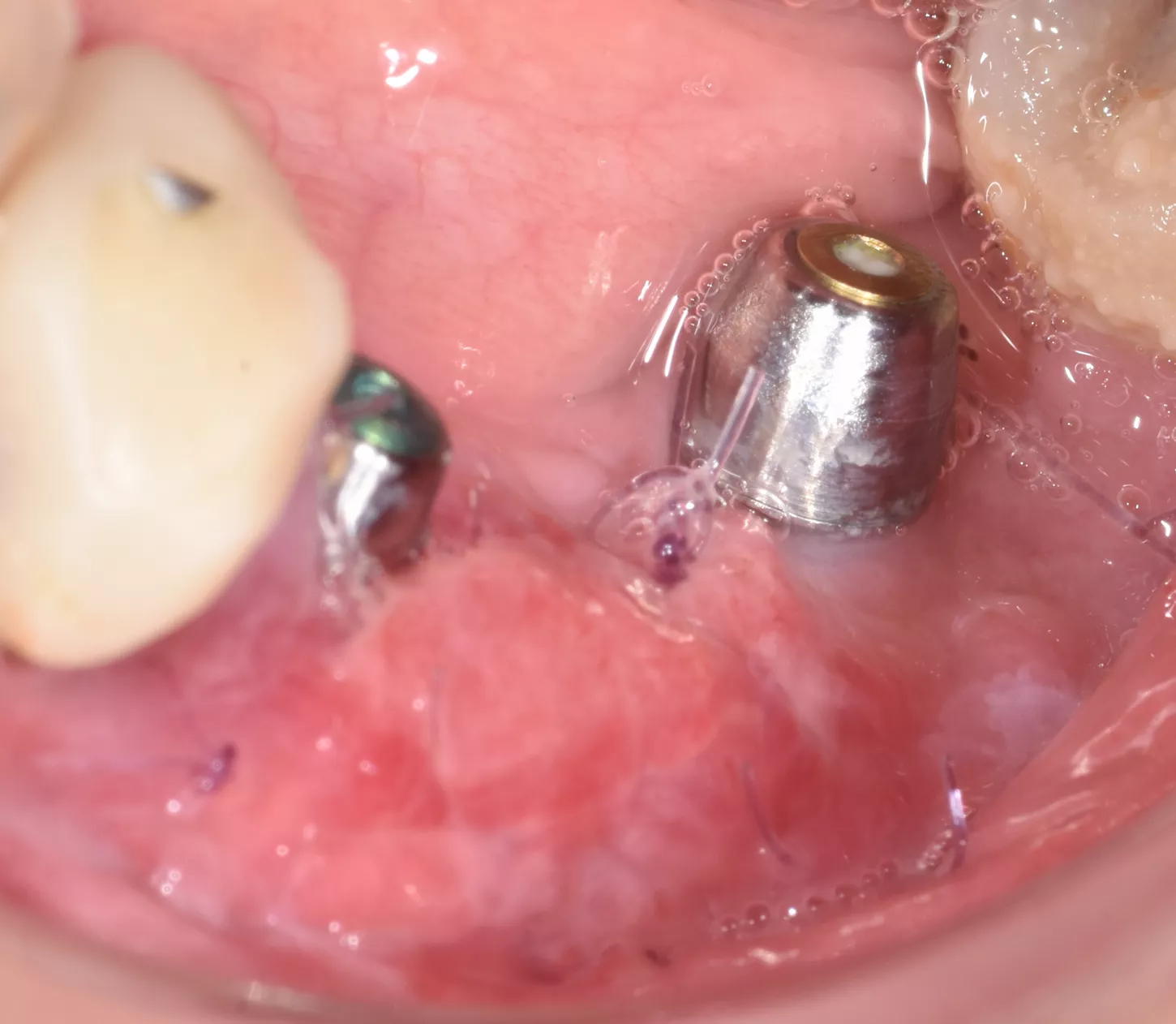
7. 3 months later: to increase the amount of keratinised tissue, connective epithelial graft with positioning of 2 multi-unit abutments with on the implants was done. ISQ 75.
8. 10 days later, satisfactory healing of the mucogingival procedure.
Final situation:
9. Panoramic control 2 years after the implants were put into service.

10. Clinical situation 2 years later with the crowns screwed onto the MU abutments (Dr S. Abid, Nice).

Conclusion:
The autogenous split bone block technique offered interesting indications and results in terms of regenerated bone volume which can be attributed to a combination of the short healing period of 5 months, which was sufficient for revascularization of the graft and the secure insertion of dental implants [3].
Two years after the surgical procedures, stable bone regeneration was observed, the implants were osseointegrated and the patient maintained satisfactory oral hygiene.
References
1. Cawood JI, Howell RA. A classification of the edentulous jaws. Int J Oral Maxillofac Surg 1988. 17(4): pp. 232–6.
2. Chiapasco M, Casentini P, Zaniboni M. Bone augmentation procedures in implant dentistry. Int J Oral Maxillofac Implants 2009. 24 Suppl: pp. 237–59.
3. Sakkas A, Wilde F, Heufelder M, Winter K, Schramm A. Autogenous bone grafts in oral implantology—is it still a “gold standard”? A consecutive review of 279 patients with 456 clinical procedures. Int J Implant Dent 2017. 3(1)
4. Chiapasco M, Zaniboni M, Boisco M. Augmentation procedures for the rehabilitation of deficient edentulous ridges with oral implants. Clin Oral Implants Res 2006. 17(S2): pp. 136–159.
5. Cordaro L, Torsello F, Ribeiro CA, Liberatore M, Torresanto VMd. Inlay-onlay grafting for three-dimensional reconstruction of the posterior atrophic maxilla with mandibular bone. Int J Oral Maxillofac Surg 2010. 39(4): pp. 350–7.