





















Simultaneous sinus lift and implant rehabilitation of severe bone resorption in the posterior maxillary quadrant using Axiom X3® Bone Level.

Dr. Romain CASTRO
QUALIFIED SPECIALIST IN ORAL SURGERY
France
- Private practice, ICOI Institut de Chirurgie Orale et d'Implantologie, Clinique Juge 13008 Marseille
- Part-time hospital practitioner, Centre hospitalier Edmond Garcin, 13400 Aubagne.
- Former intern at the Hospitals of Marseille and Nice
- Former Assistant at the Hospitals of Marseille
- President of ACOSE (Association of South-East Oral Surgeons).
- Scientific Co-Director of the University Diploma in Pre-implant Bone Surgery (DU COPI), IUFC, CHU NICE.
Case introduction:
The clinical case involves a 59-year-old patient with no prior health issues.
The corresponding dentist (Dr. Brière Mathieu) requested a fixed rehabilitation in the maxillary posterior section to replace the missing tooth 16.
From a prosthetic perspective, it was decided, with the patient's agreement, to rehabilitate 16 and maintain a 'short arch' without replacing the second molars.
Upon examination, it was found that the patient had a broad crest and thick periodontal tissue with satisfactory gingival height. A cone beam examination confirmed that the width of the bone crest was 10.8 mm. However, the residual bone height was only 2.8mm, which was deemed insufficient for the planned implant (Axiom® BL X3 Ø 4mm, length 10mm) without hard tissue augmentation. Nonetheless, implant placement with a concomitant sinus lift can be considered when bone heights are ≥ 2 mm [1-4]. As a result, a surgical decision was made to place an Axiom X3® Bone Level implant to replace 16, along with a simultaneous sinus lift to facilitate both implant placement and bone regeneration in one procedure.
The diameter of the implant is consistent for the replacement of a molar in terms of emergence profile and mechanical strength. The 10 mm length allows a ‘tenting effect’ to be achieved, supporting the detached sinus mucosa which rests on the implant apex. The implant, along its entire length, will then act as a support for the biomaterial impregnated with the blood clot, allowing the bone to regenerate [5].
Initial situation
1. Pre-operative clinical view
The occlusal view shows a ridge with a satisfactory width and a thick, healthy periodontal phenotype.

2a. 2b. Pre-operative CBCT scan :
Crestal bone dimensions width 10.8 mm and height: 2.8 mm.


The Alpha angle, formed by the anterior lateral wall of the maxillary sinus and the palatal wall, is favorable at > 60° [1].
The thickness of the sinus mucosa is favorable > 1.5 mm, indicating a limited risk of perforation. Thickening is not pathological in this patient.
The thickness of the vestibular bone wall is normal, between 1 and 2.5 mm. No intra-sinus septum.
The Beta angle, formed by the palatal wall of the maxillary sinus and the inter-sinus-nasal septum, is on the other hand very closed, which may entail risks in the detachment of the mucosa in this area.
Surgical procedure:
3. Flap detachment:
Crestal incision and diverging vertical discharges. Mucoperiosteal lift.
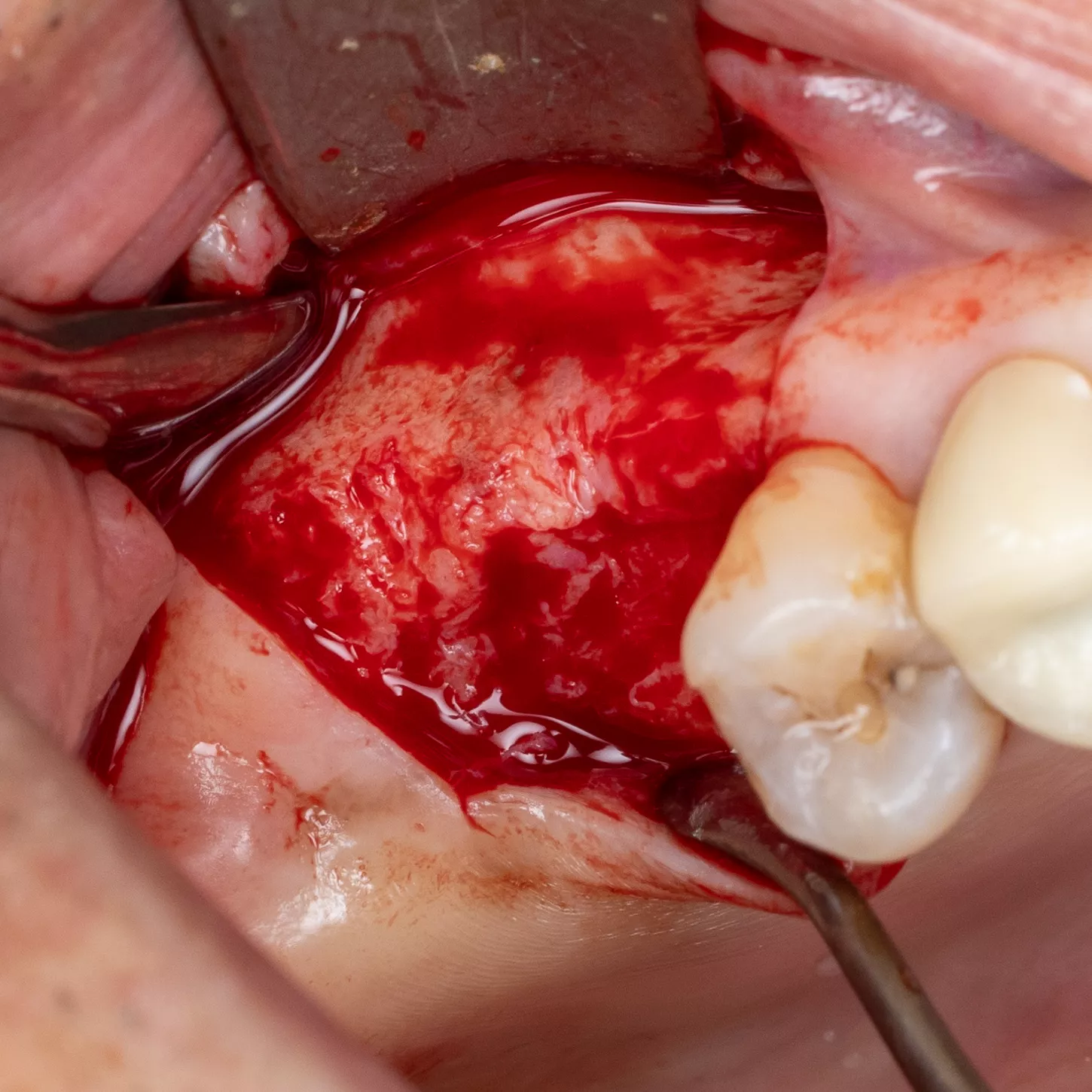
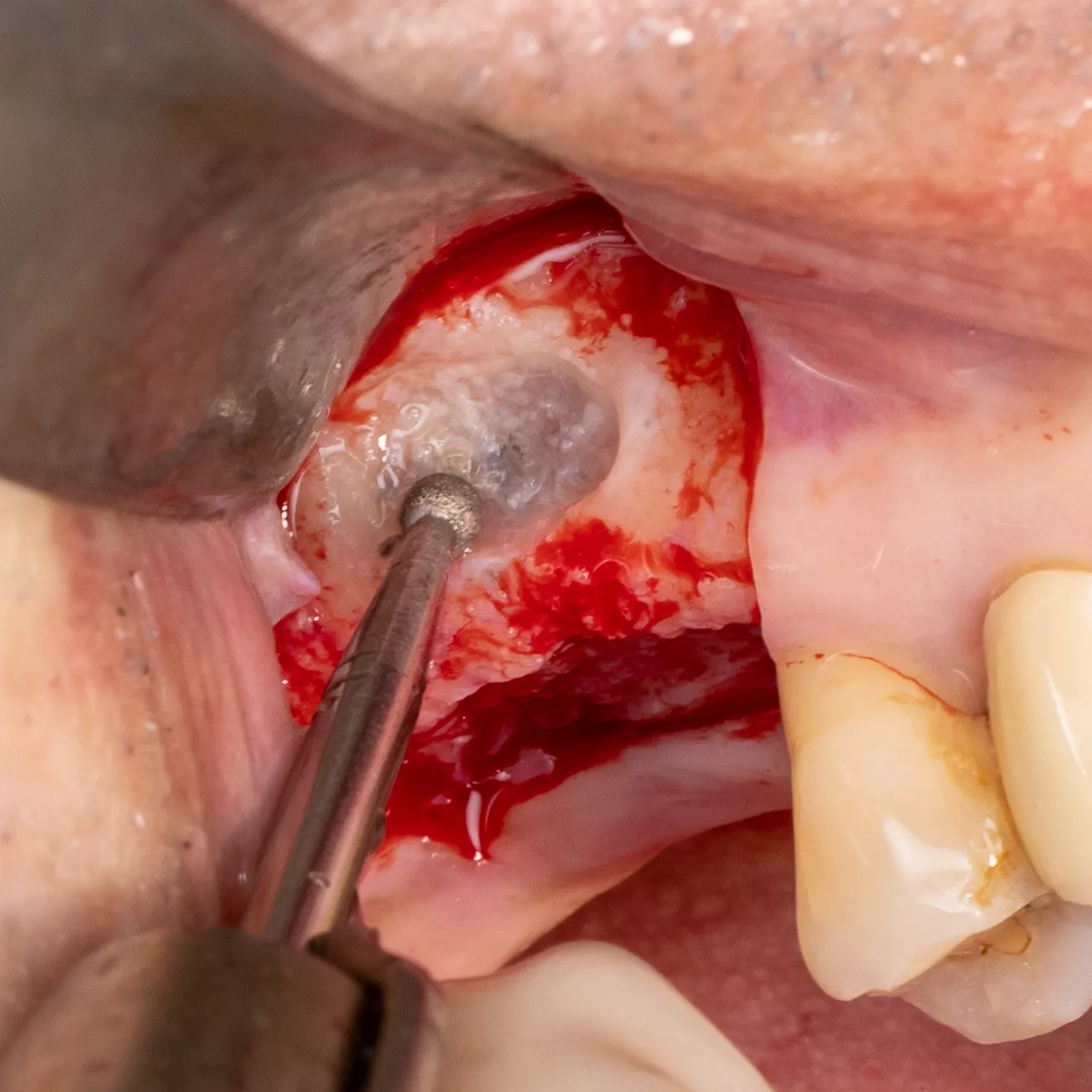
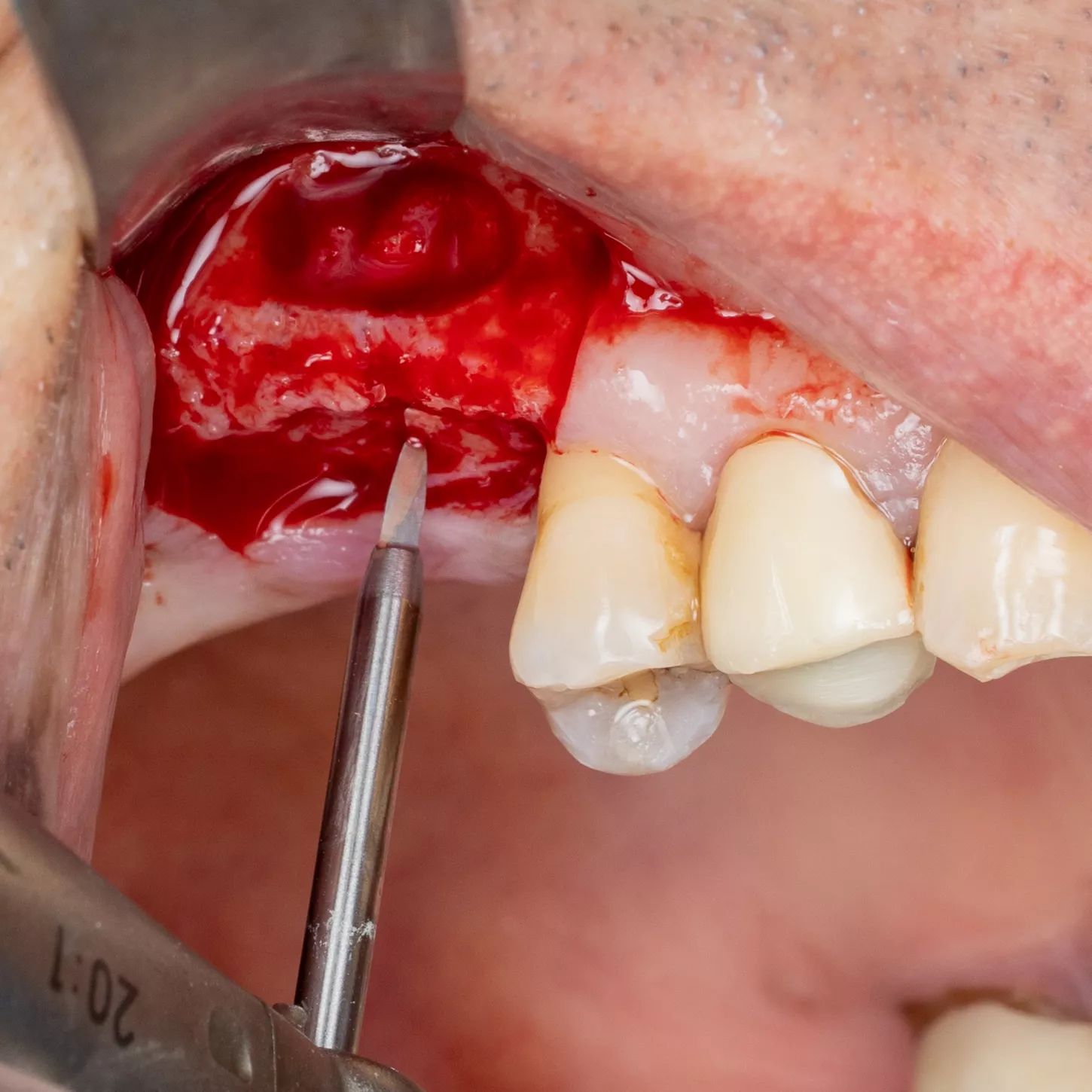
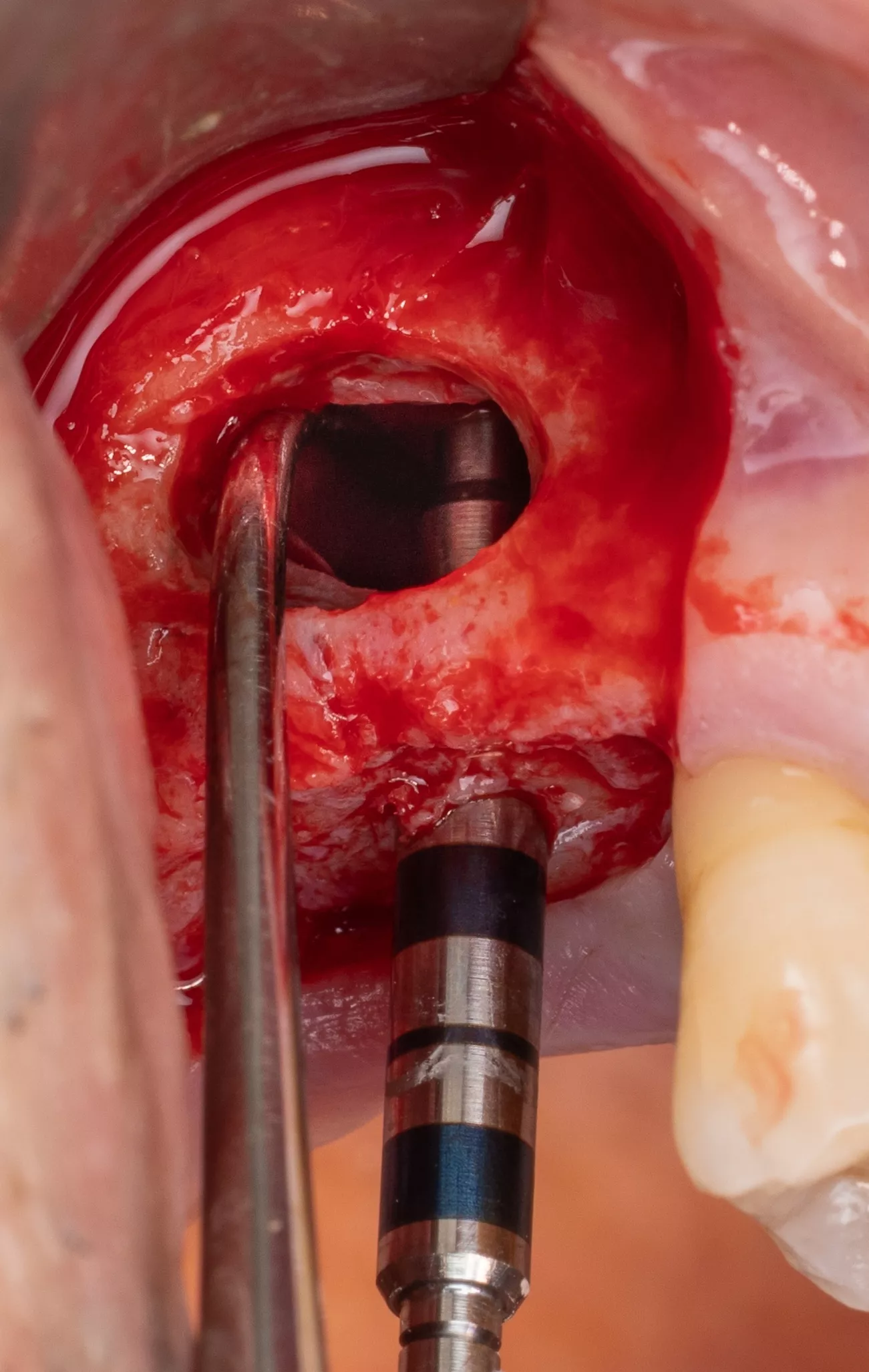
4. Sinus window : Subtractive osteotomy without preservation of the bone flap using a 2.5 mm diamond bur mounted on a surgical handpiece. The Schneiderian membrane (sinus mucosa) of slightly bluish grey color is exposed.
5. Initiation of lifting of the sinus mucosa through the inferior mesial window angle.
6. Placement of a saline-impregnated collagen sponge to assist the detachment by conferring increased but gentle and evenly distributed pressure.
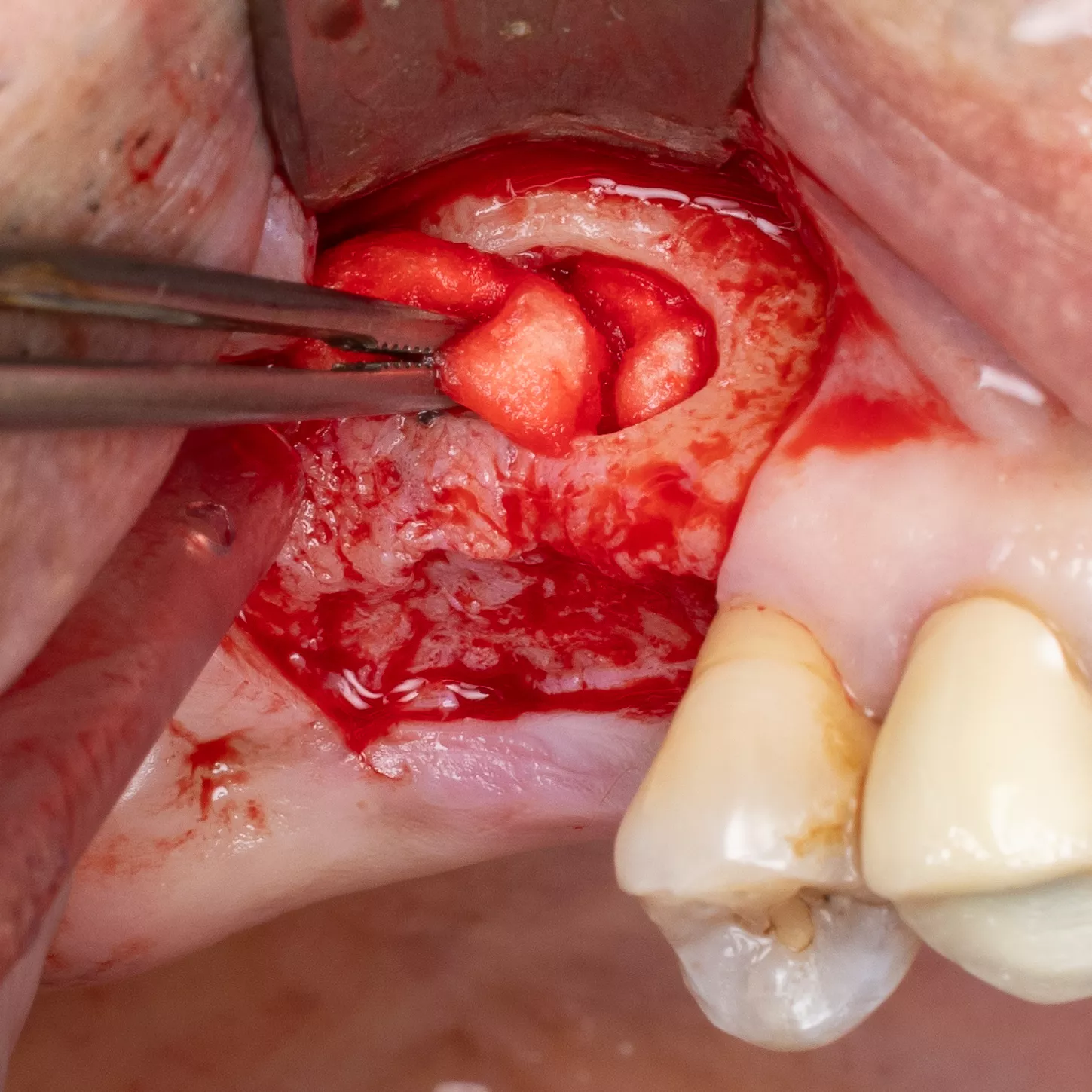
7. Sinus mucosa detached.

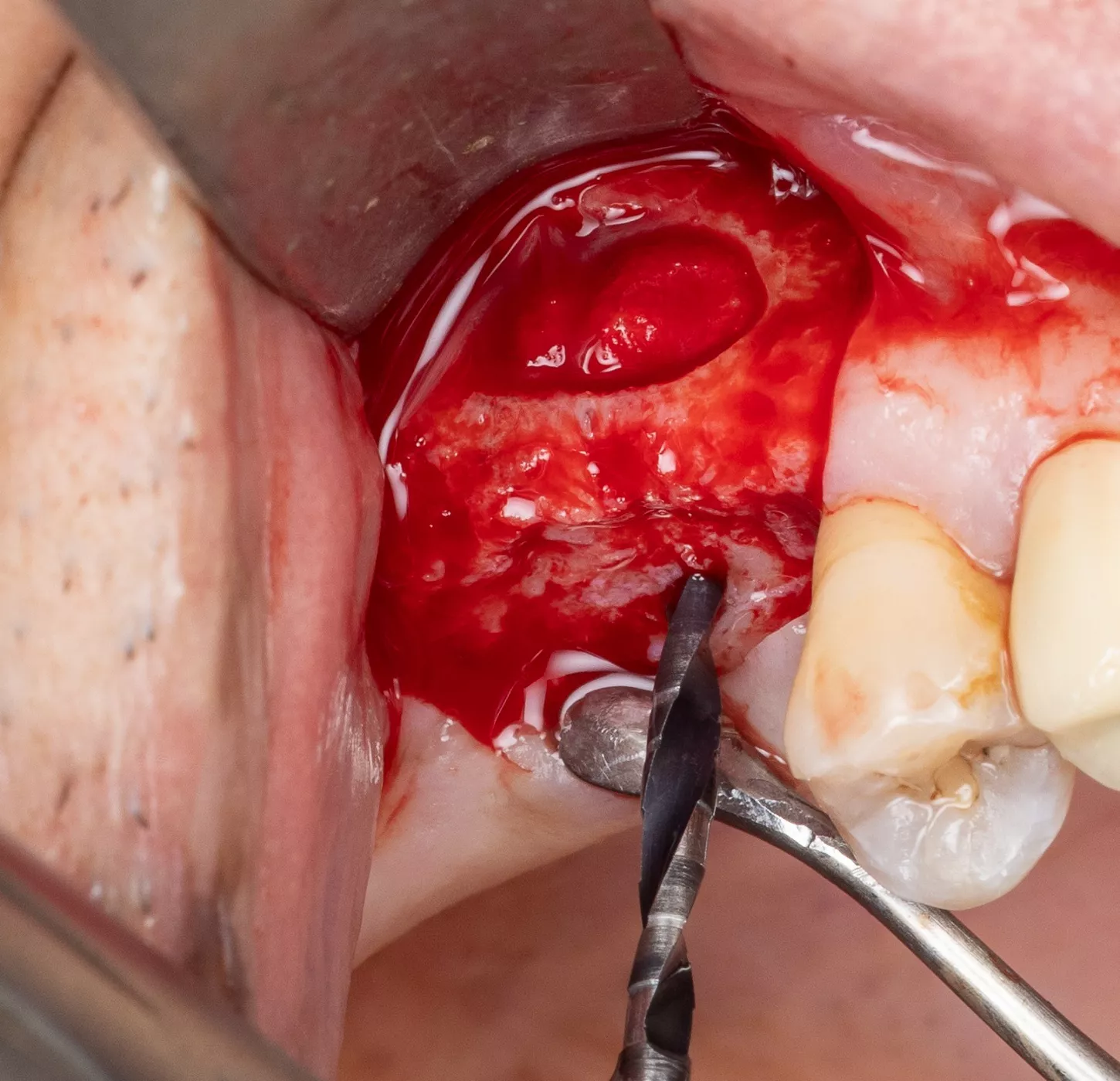
8. Verification of the absence of mucosal adherence at the Beta angle and at the inter-sinus-nasal septum using a Freer sinus elevator.

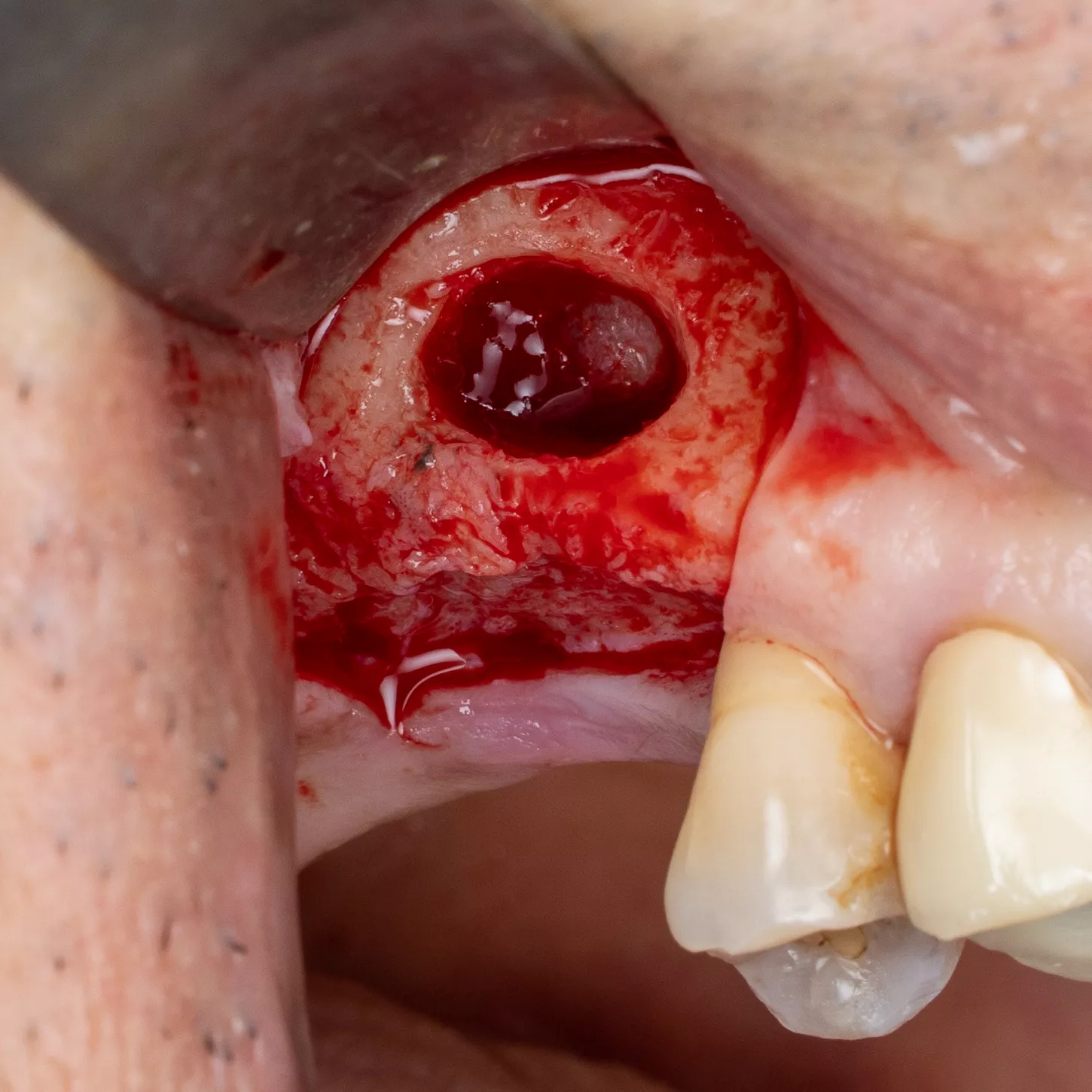
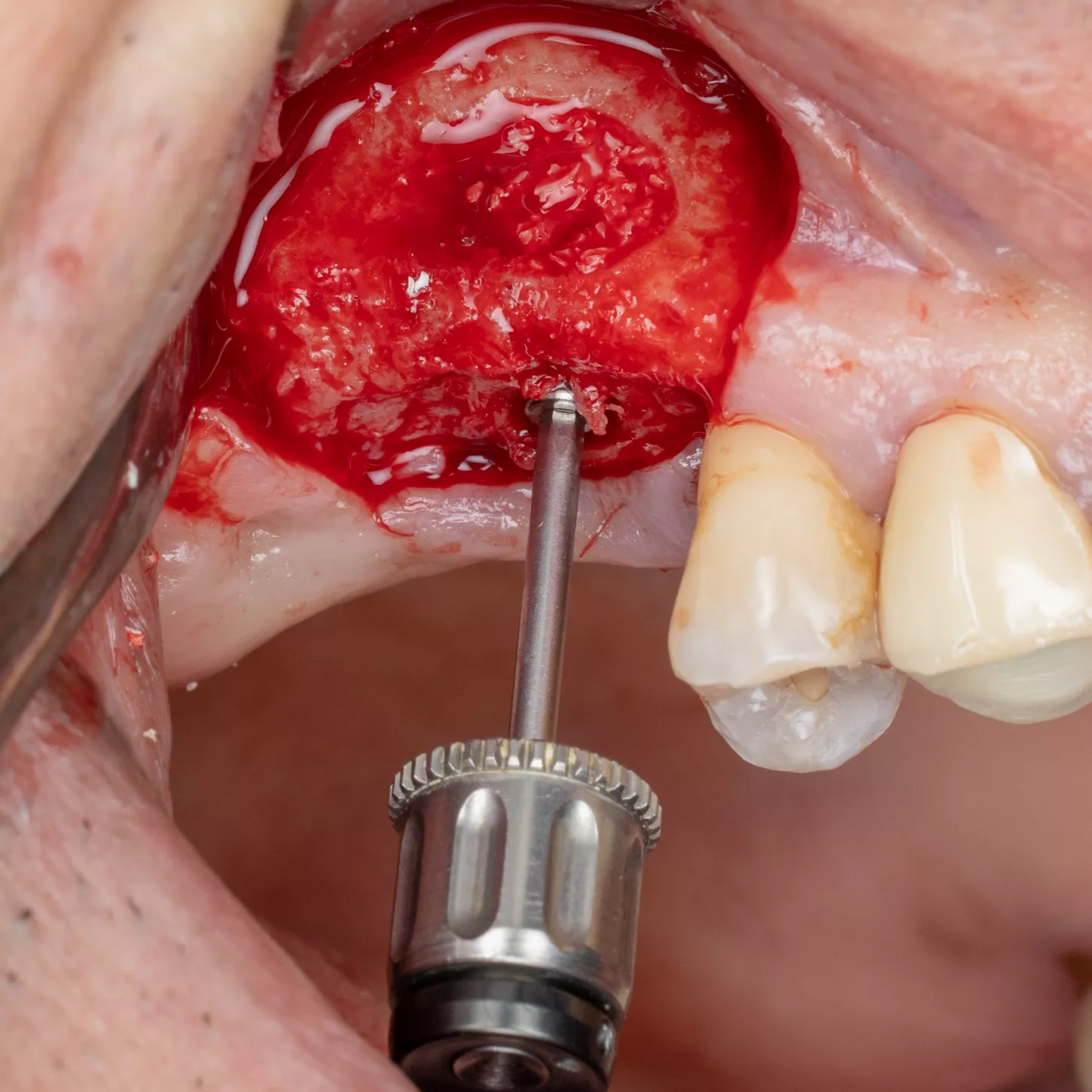
9. Placement of a new collagen sponge to protect the mucosa from the drill holes and start of the implant drilling sequence with the Pointer drill.
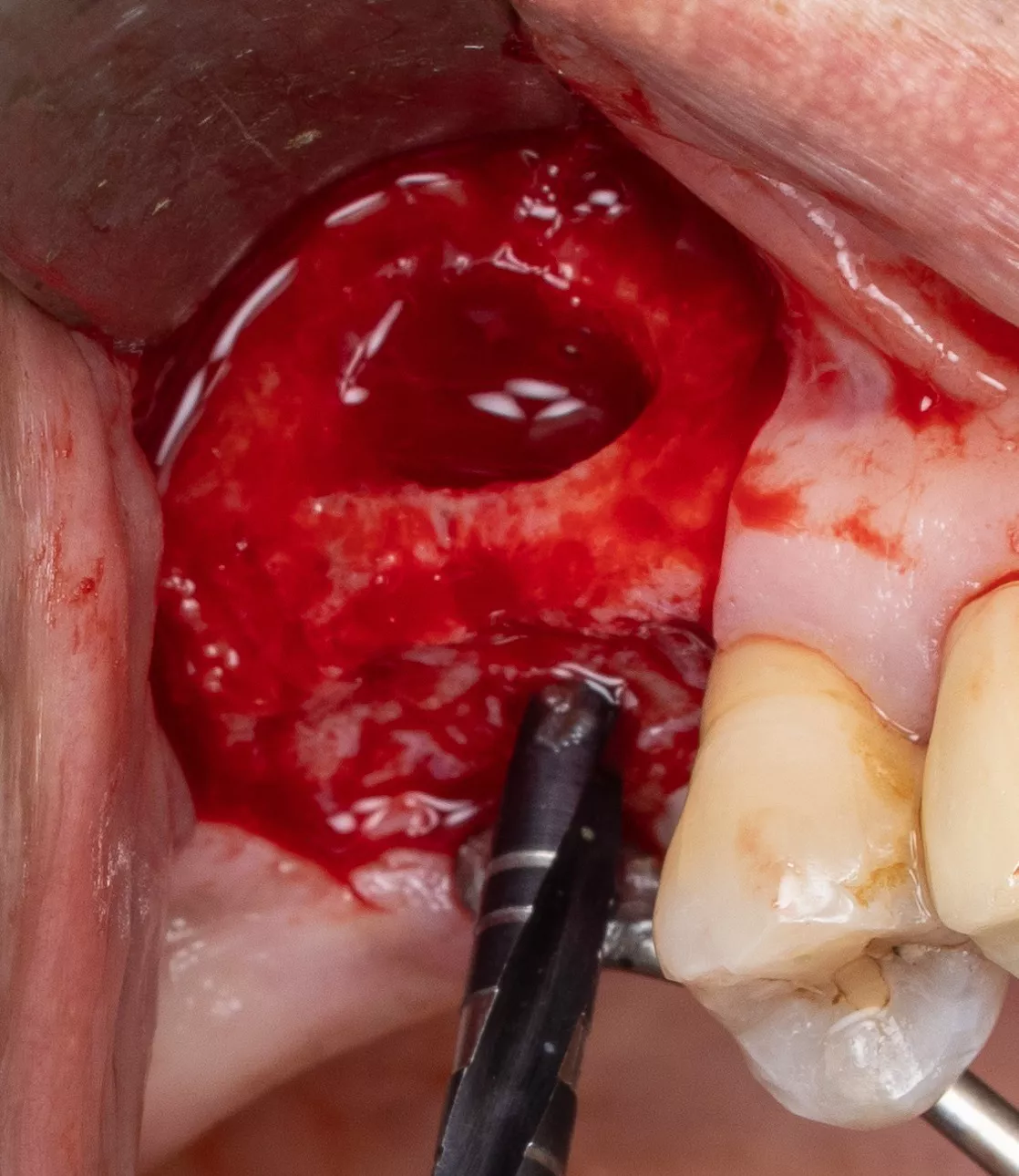
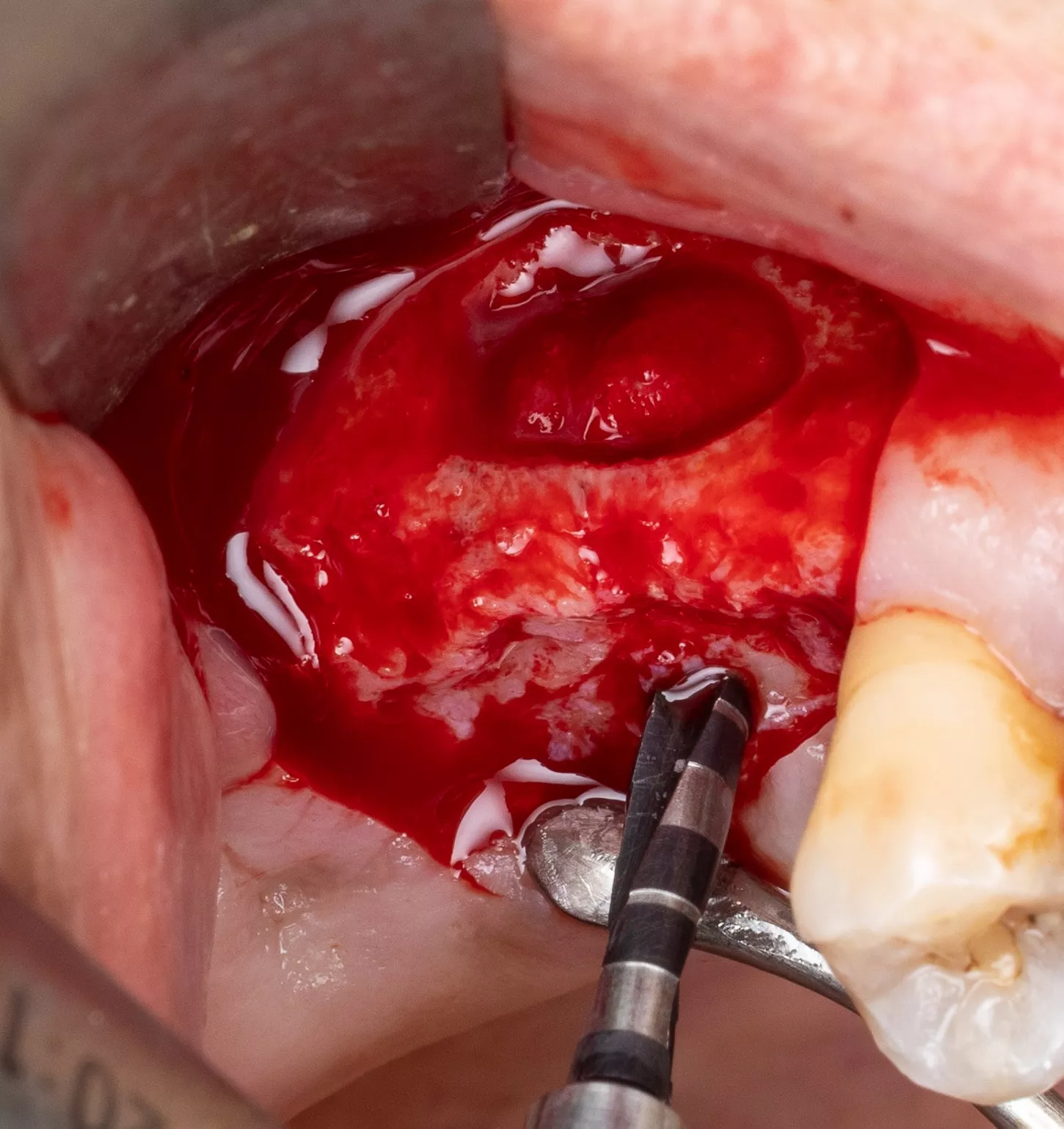
10, 11, 12, 13, 14, 15:
Drilling sequence and control of implant axis with gauges corresponding to the diameter of the drills used, all included in the surgical kit Axiom®.
10. Sequential drilling using an initial Ø 2 mm drill, followed by a Ø 2.4 mm drill (green).
14. The last drill used has a Ø 3.0 mm diameter (red), for the placement of Axiom® BL X3 Ø 4.0 mm and 10mm length implant and confirmation of the axis using the adapted gauge.
11. 12. 13. Checking the depth and axis using the gauge.
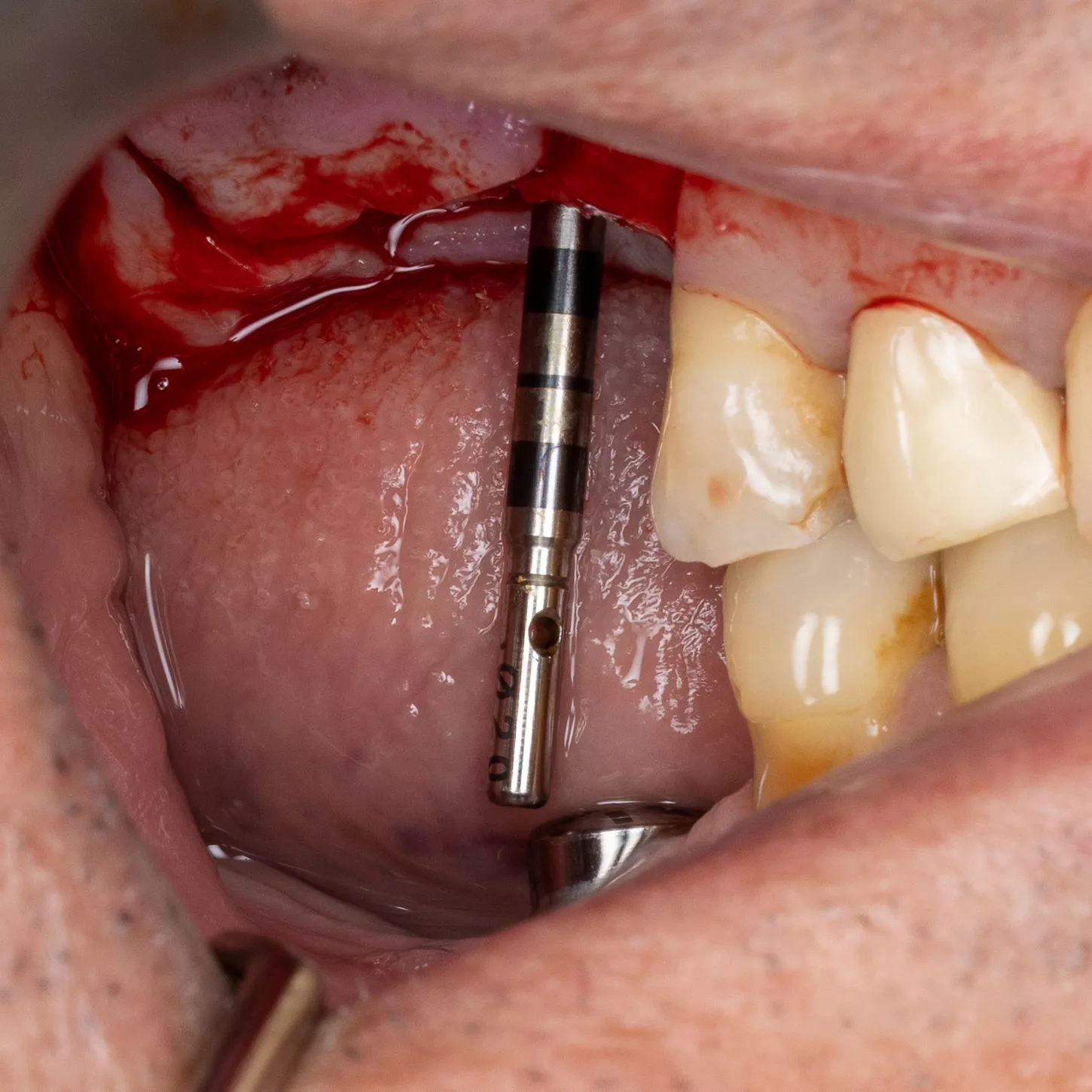

15.
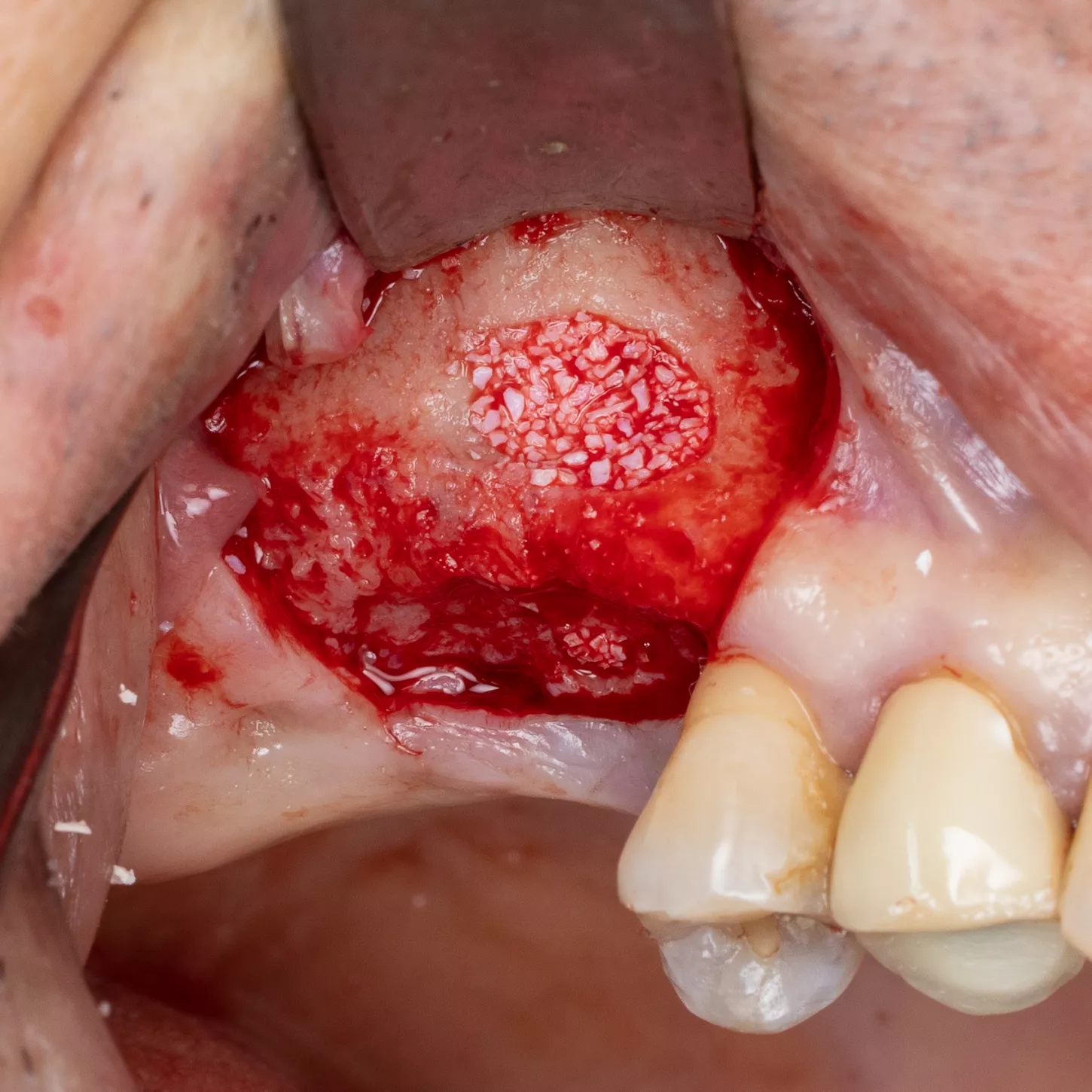
16. Prior to implant placement, filling of the palatal and mesial area of the sinus cavity with axenogenic biomaterial (XenoGraft, Straumann®).

17. Filling and compression using a graft packer in the mesio-palatal direction.
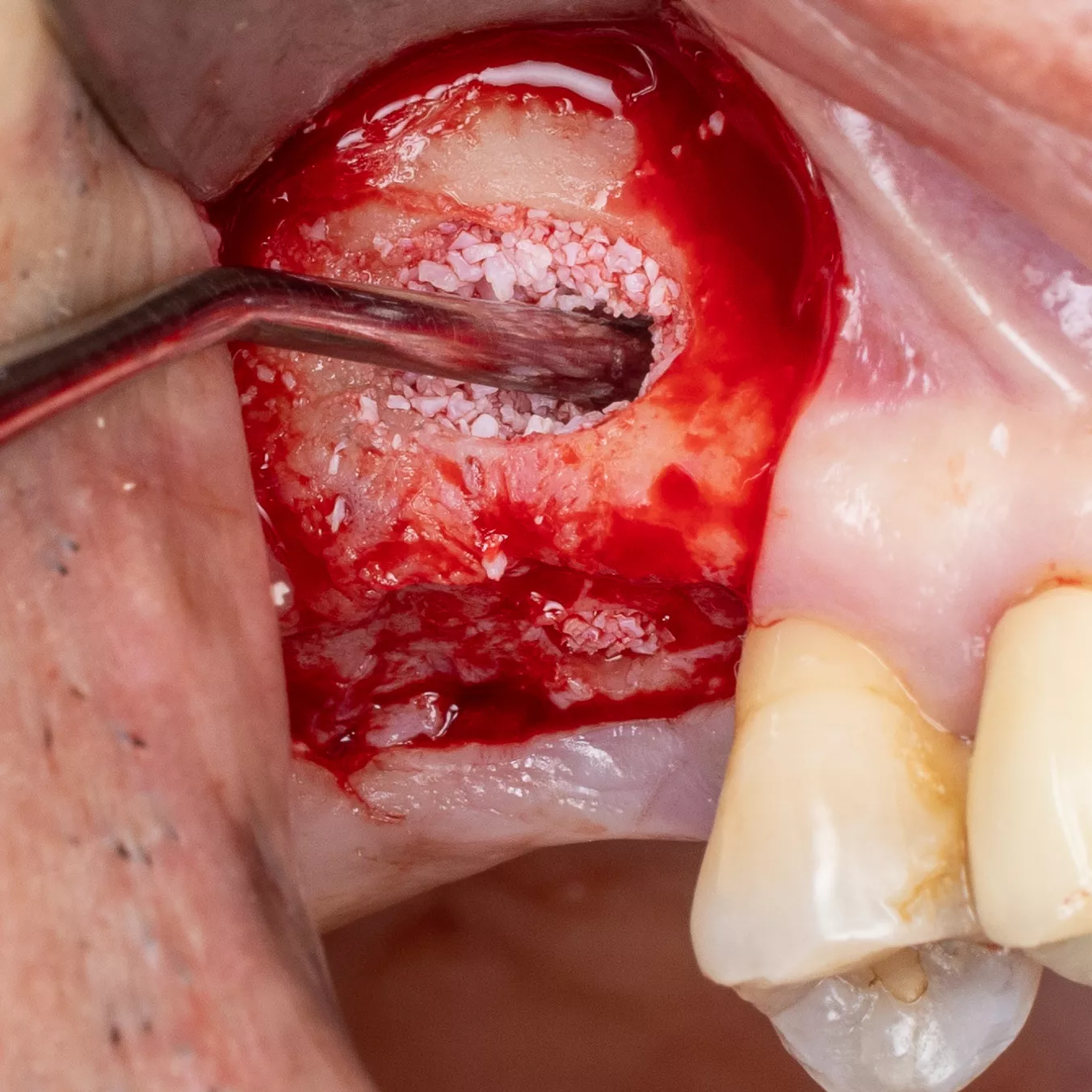
18. The sinus cavity is densely packed with the bone graft composite to support the implant.
19. The Anthogyr Axiom® BL X3 Ø 4.0 mm, length 10 mm implant is inserted.
20. Verification of correct positioning of the implant at a depth 1 mm below the crest of the bone.
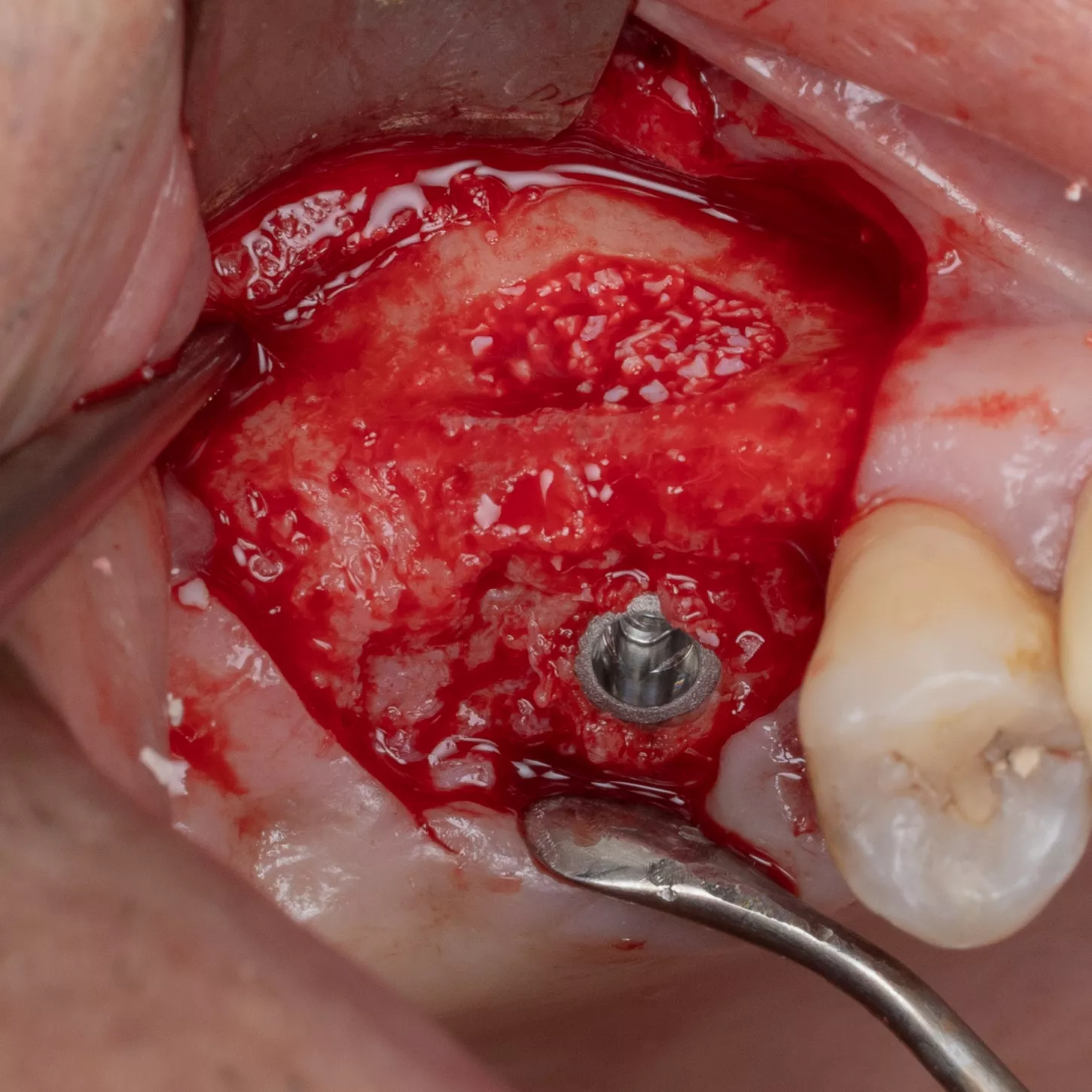
21. Placement of the cover screw tightened by hand using a screw wrench.
22. Post-operative X-ray.
Bone consolidation and a close relationship between bone and implant with a tenting effect by the implant can be observed.

Prosthetic restoration:
23. Placement of the healing abutment and final prosthesis.
Nota bene: The healing phase, involving the placement of Ø 6mm, 4mm gingival height healing screw after submerged healing for 5 months was not documented in images. After this period, there was a 3-week waiting period before the patient's appointment to have the prosthesis made by Dr. Brière Mathieu, the corresponding dental surgeon.

24. 25. 25. 27.
Clinical views of the implant-supported prosthesis 4 months after fitting. Lateral views in occlusion and occlusal views.



Conclusion :
It is crucial that implant placement is preceded by a thorough presurgical evaluation and para-clinical assessment before sinus lift surgery. In this case of severely atrophic maxilla with less than 3 mm of residual alveolar bone height, successful treatment involved sinus floor augmentation and bone regeneration with simultaneous implant placement. The use of taper designed implants and adapted surgical techniques was instrumental in achieving successful results [1-4]. The Axiom X3® Bone Level implant and the Axiom® surgical kit possess the necessary qualities for such procedures. Success in this type of treatment depends on compliance with the sequential drilling protocol and a comprehensive understanding of the system. Implementing these 1-stage surgical protocols is demanding but can significantly reduce treatment time for patients and allow for a less invasive approach, ultimately leading to higher patient satisfaction.
References
1. Antoun H, Pereira S, Zouiten O, Pereira S. Greffe de sinus par abord latéral associée à une greffe allogénique en onlay. Un cas de classe V. Rev_Odont_Stomat_2016_45_p55-66. 2016.
2. Cha H-S, Kim A, Nowzari H, Chang H-S, Ahn K-M. Simultaneous Sinus Lift and Implant Installation: Prospective Study of Consecutive Two Hundred Seventeen Sinus Lift and Four Hundred Sixty‐Two Implants. Clin Implant Dent Relat Res 2014. 16(3): pp. 337–347.
3. Michael P, Ziv M, Gavriel C, K. GA. Sinus Floor Augmentation with Simultaneous Implant Placement in the Severely Atrophic Maxilla. J Periodontol 1998. 69(12): pp. 1397–1403.
4. Mahmoud A-D. Recent Trends in Sinus Lift Surgery and Their Clinical Implications. Clin Implant Dent Relat Res 2016. 18(1): pp. 204–212.
5. Song D-S, Kim C-H, Kim B-J, Kim J-H. Tenting effect of dental implant on maxillary sinus lift without grafting. J Dent Sci 2020. 15(3): pp. 278–285.